Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Differential diagnosis of intraspinal and extraspinal non-discogenic sciatica
Available online at www.sciencedirect.com
Journal of Clinical Neuroscience 15 (2008) 1246–1252
Differential diagnosis of intraspinal and extraspinal
non-discogenic sciatica
Duygu Geler Kulcu a,*, Sait Naderi b
a Department of Physical Medicine and Rehabilitation, Yeditepe University School of Medicine, Yeditepe University Hospital,
Devlet Yolu Ankara Caddesi No. 102/104 Kozyatag˘ı, Istanbul, Turkey
b Department of Neurosurgery, Yeditepe University School of Medicine, Istanbul, Turkey
Received 10 December 2007; accepted 5 January 2008
The aim of this study is to present a series of 11 patients with non-discogenic sciatica (NDS), and to review the diagnostic techniques
of careful clinical and radiological examination. The cases include lumbar radicular herpes zoster, lumbar nerve root schwannoma,lumbar instability, facet hypertrophy, ankylosing spondylitis, sacroiliitis, sciatic neuritis, piriformis syndrome, intrapelvic mass andcoxarthrosis. The pain pattern and accompanying symptoms were the major factors suggesting a non-discogenic etiology. PelvicMRI and CT scans, and sciatic nerve magnetic resonance neurography were the main diagnostic tools for diagnosis of NDS. The treat-ment of choice depended on the primary diagnosis. Detailed physical examinations with special attention paid to the extraspinal causesof sciatica and to pain characteristics are the major components of differential diagnosis of NDS.
Ó 2008 Elsevier Ltd. All rights reserved.
Keywords: Magnetic resonance neurography; Non-discogenic sciatica; Piriformis syndrome; Sacroiliitis; Sciatica
NDS, and overviews the different causes of intraspinaland extraspinal sciatica.
Sciatica is common, and is frequently caused by lumbar
disk herniation.However, some intraspinal or extraspinal
pathologic processes along the sciatic nerve may also causesciatica. Whereas lumbar spine imaging reveals the causes
The patients, 6 female and 5 male, were aged between 25
of intraspinal non-discogenic sciatica (NDS), extraspinal
and 65 years old. There were 4 patients with extraspinal
sciatica is often misdiagnosed because routine diagnostic
NDS, 4 with intraspinal NDS, and 3 with sciatica second-
tests focus on the lumbar Extrapelvic causes affect
ary to both spinal and extraspinal processes.
the nerve as it progresses distally from the sciatic notch.
A careful patient history and clinical examination are
2.1. Intraspinal non-discogenic sciatica
important in identifying extraspinal sciatica. Further diag-nostic imaging may clarify the diagnosis.
2.1.1. Lumbar radicular herpes zoster (Patient 1)
In general, studies of NDS tend to focus on only one dis-
A 64-year-old woman was admitted with a 1-week his-
order.This study reports a series of 11 patients with
tory of left leg pain that was not responding to analgesics.
A neurological examination revealed no abnormal findings.
A lumbar MRI showed degenerative changes A
physical examination revealed typical skin lesions along
Corresponding author. Tel.: +90 216 5784100; Mob.: +90 505
the L3 and L4 dermatomes The patient was re-
E-mail address: (D.G. Kulcu).
ferred to the dermatology department, where the lesions
0967-5868/$ - see front matter Ó 2008 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jocn.2008.01.017

D.G. Kulcu, S. Naderi / Journal of Clinical Neuroscience 15 (2008) 1246–1252
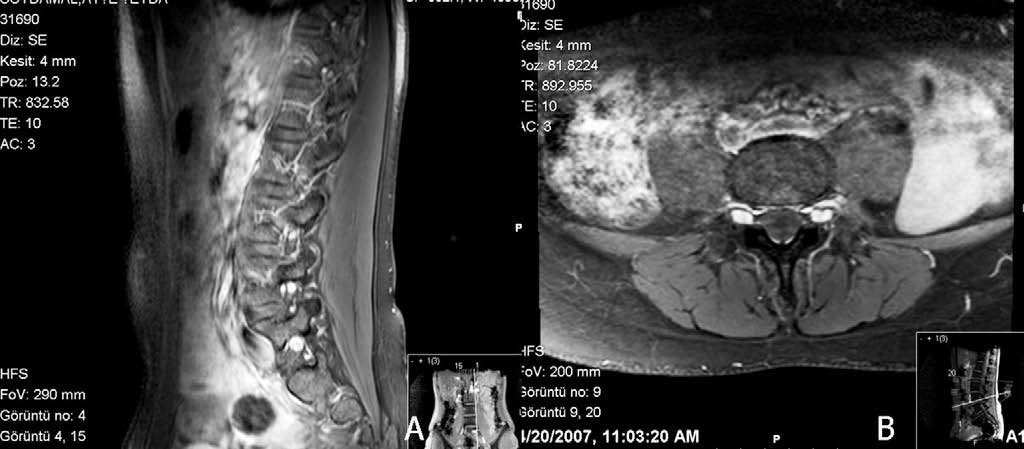
Fig. 1. (A) Sagittal T1-weighted lumbar MRI showing degenerative changes. (B) Skin lesions along the trajectories of the L3 and L4 nerve roots.
Fig. 2. (A) Sagittal postcontrast T1-weighted lumbar MRI, and (B) axial fat-saturated T1-weighted lumbar MRI showing multiple schwannomatosis.
were determined to be caused by herpes zoster. After
tive. The patient had pain with extension of the trunk.
receiving medication for herpes zoster, the patient's symp-
There was no neurological deficit. A lumbosacral antero-
toms resolved.
posterior (AP) radiograph showed sclerotic and degenera-tive changes in the L5–S1 facet joint on the left side. A
2.1.2. Schwannomatosis (Patient 2)
lumbar MRI showed a L4–L5 and L5–S1 central disc pro-
A 27-year-old female patient was admitted with a 2-
trusion. After physical therapy and flexion exercises, the
month history of low back pain (LBP) and left leg pain.
symptoms resolved partially.
Physical examination revealed a positive straight leg raising(SLR) test at 45°, and hypoesthesia at the left S1 derma-
2.1.4. Lumbar instability (Patient 4)
tome. Lumbar MRI showed multiple schwannomatosis of
A 31-year-old male was admitted with a 12-year history
the bilateral L5 and left S1 nerve roots (). The symp-
of LBP and a 1-month history of left leg pain. Physical
toms improved after medical therapy. Because of the lack
examination showed a positive SLR test at 60°. The patient
of neurological deficit and the small size of the schwanno-
was mistakenly diagnosed as having a lumbar disc hernia
mas, surgical treatment was not indicated.
(LDH) at another center and was treated with physiother-apy, which was not beneficial. Sagittal lumbar MRI
2.1.3. Facet syndrome and lumbar disk herniation
showed no disc herniation, and axial MRI showed pars de-
fects of L5. Oblique radiographs showed bilateral pars int-
A 63-year-old woman was admitted with a history of
erarticularis defects. The LBP was attributed to the lumbar
LBP, left leg pain and numbness. The SLR test was nega-
instabilty related to the isthmic defects.
D.G. Kulcu, S. Naderi / Journal of Clinical Neuroscience 15 (2008) 1246–1252
2.2. Extraspinal cases
nerve root compression and bilateral sacroiliitis. Thesciatica was attributed to the sacroiliitis. The patient reci-
2.2.1. Sciatic neuritis (Patient 5)
eved indomethacin at 150 mg/day for 15 days. The
A 64-year-old woman was admitted to hospital with left
patient's symptoms resolved. The visual analogue scale
buttock pain. The patient had undergone surgery for lum-
(VAS) pain score decreased from 7 to 2. Further analyses
bar spondylolisthesis 10 years previously. The results of a
were performed to identify the etiology of the sacroiliitis
physical examination were unremarkable. A lumbar MRI
showed left sciatic neuritis between the piriformis muscle
and the proximal femur ).
2.2.3. Sacroiliitis (Patient 7)
2.2.2. Bilateral sacroiliitis (Patient 6)
A 53-year-old woman was admitted with left leg pain.
A 25-year-old female was admitted with a 2-month his-
Physical and neurological examinations yielded no abnor-
tory of LBP, left-side buttock and posterior thigh pain. The
mal findings. Lumbar MRI showed no abnormality. Sacro-
patient had no lower limb weakness or paresthesias and
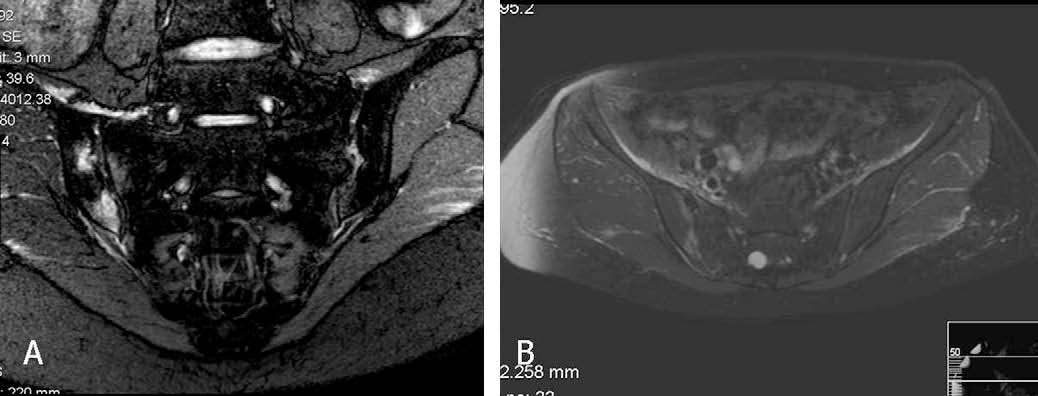
iliac MRI showed sacroiliitis and edema in the joint
had no history of morning stiffness or night pain. On phys-
compressing the sciatic nerve ). The erythrocyte sed-
ical examination the SLR test was limited to 60° on the left
imentation rate (ESR) was 88 mm/h. After further exami-
side. There was no other neurologic deficit in the lower
nation, the patient was diagnosed with seronegative
limbs. Her range of motion of the trunk was not limited
spondyloarthropathy. The patient started to recieve indo-
and was not painful. Deep palpation of the left buttock
methacin at 300 mg/day, salazosulphapyridine at 400 mg/
over the sciatic nerve course was painful. Gaenslen's test
day and prednisolone acetate at 7.5 mg/day. Pain de-
was positive on the left side. The sacroiliac compression
creased and the ESR was 68 mm/h after 2 weeks. Symp-
test was positive on the left side. MRI of the lumbar spine
toms completely resolved after completion of the medical
and sacroiliac joint showed L4–L5 disc protrusion with no
2.2.4. Soft tissue tumor (Patient 8)
A 55-year-old male was admitted with a 1-month history
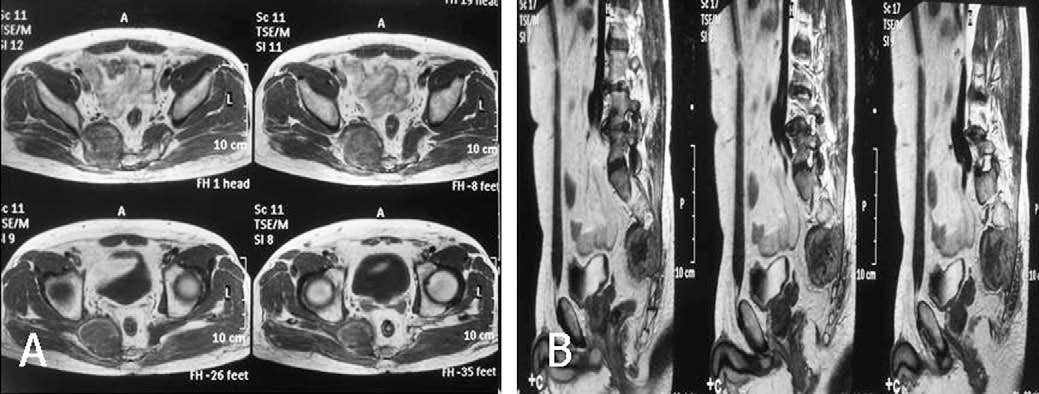
of right buttock pain. The patient had undergone L4–L5discectomies five and three years previously. Neurologicalexamination revealed no deficit. The buttock was painfulupon palpation. Lumbar spine MRI showed modicchanges at the L4–L5 level. A pelvic MRI showed a 6 cmsoft tissue mass anterior and right to the sacrum. Examina-tion of a pelvic CT scan revealed destruction of the anteriorsurface of the sacrum (A CT-guided needle biopsyrevealed an angiosarcoma.
2.2.5. Piriformis syndrome and hamstring tendinopathy(Patient 9)
A 59-year-old woman was admitted with a 2-month his-
tory of left-side buttock and posterior thigh pain. The pa-tient had an antalgic gait with knee flexed and hip
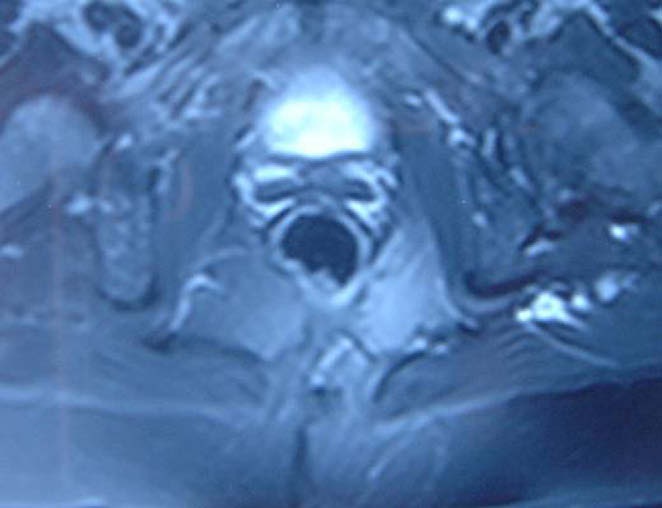
Fig. 3. Axial fat saturated T2-weighted lumbar MRI showing hyperin-
adducted and was not able to walk further than 10 m
tensity at the left sciatic nerve.
Fig. 4. (A) Coronal STIR-weighted and (B) axial postcontrast fat-saturated T1-weighted sacroiliac joint MRIs showing inflammation on the left side.

D.G. Kulcu, S. Naderi / Journal of Clinical Neuroscience 15 (2008) 1246–1252
Fig. 5. (A) Axial postcontrast T1-weighted and (B) sagittal T2-weighted pelvic MRIs revealing a 4 cm � 5 cm soft tissue tumor right and anterior to thesacrum.
partially but the patient still complained of left thigh painafter prolonged sitting and hip internal rotation. MRIneurography showed no abnormal signal at the sciaticnerve. The patient underwent a tetracosactrin injectionprotocol but received no benefit. A new examination re-vealed negative SLR. Freiberg's sign was positive at theleft side. Although MRN showed no abnormality, giventhe results of a physical examination, the patient wasdiagnosed as having PS and the physical therapy protocolfor PS was applied.The patient received 15 sessions of
Fig. 6. (A) Axial T1-weighted pelvic magnetic resonance neurography
physical therapy. At the end of the physical therapy
(MRN) showing left piriformis muscle asymmetry and atrophy, and (B)
regimen, the VAS score decreased from 9 to 2 points.
axial postcontrast fat-saturated T1-weighted pelvic MRN showing leftischial bone marrow edema and hamstring tendinopathy. Note that the
The patient was comfortable after prolonged sitting and
left arrow in (A) shows an atrophic and asymmetric piriformis muscle, and
internal rotation of the hip.
the arrow in (B) shows bone marrow edema and tendinopathy.
2.2.7. Degenarative lumbar spine and coxarthrosis (Patient11)
because of increasing symptom intensity. At physical exam-
A 65-year-old male was admitted with bilateral buttock
ination the SLR test was negative. Freiberg's sign was posi-
pain and neurogenic claudication. The FABER test was
tive. The range of trunk motion was not limited. The left leg
also positive at the left side. A lumbar MRI showed L3–
was paresthetic. Tenderness in the piriformis muscle and
L4 disc herniation, lumbar spinal stenosis, and L4–L5
ischium pubis was noted on deep palpation. MRI of the
spondylolisthesis. Pelvic radiographs showed grade IV
lumbar spine yielded no abnormal findings. Magnetic reso-
osteoarthritis of the left hip. After discussion with the
nance neurography (MRN) revealed piriformis asymmetry
patient regarding a treatment plan, the patient underwent
on the left side, high signal at the sciatic nerve at this loca-
L3–4–5 decompression and instrumentation, and inter-
tion and bone marrow edema at the ischium pubis at the
transverse fusion. Two months after spinal intervention
hamstring muscle insertion site (). A physical therapy
the patient underwent total hip arthroplasty. The symp-
protocol for piriformis syndrome (PS) was applieAt the
toms resolved after surgery.
end of the physical therapy, the VAS score decreased from10 to 3 points. The antalgic gate was corrected andFreiberg's sign became negative. Tenderness of the ischium
pubis remained due to hamstring tendinopathy.
Many intraspinal and/or extraspinal pathologic pro-
2.2.6. Lumbar disc hernia and piriformis syndrome (Patient
cesses along the lumbar nerve roots and sciatic nerve can
cause sciatica. In 20% of cases, the sciatica is of both disco-
A 48-year-old male was admitted with a 6-week history
genic and non-discogenic origin.However, in practice,
of LBP and left leg pain. MRI of the lumbar spine
causes of NDS are often overlooked, partly due to the high
showed L5–S1 disc herniation compressing the left S1
nerve root. Electromyography showed S1 radiculopathy.
He underwent L5 hemipartial laminectomy, and left L5–
The causes of NDS may be classified into two major cat-
S1 microdiscectomy. After surgery, the symptoms resolved
egories: intraspinal and extraspinal. Differential diagnosis
D.G. Kulcu, S. Naderi / Journal of Clinical Neuroscience 15 (2008) 1246–1252
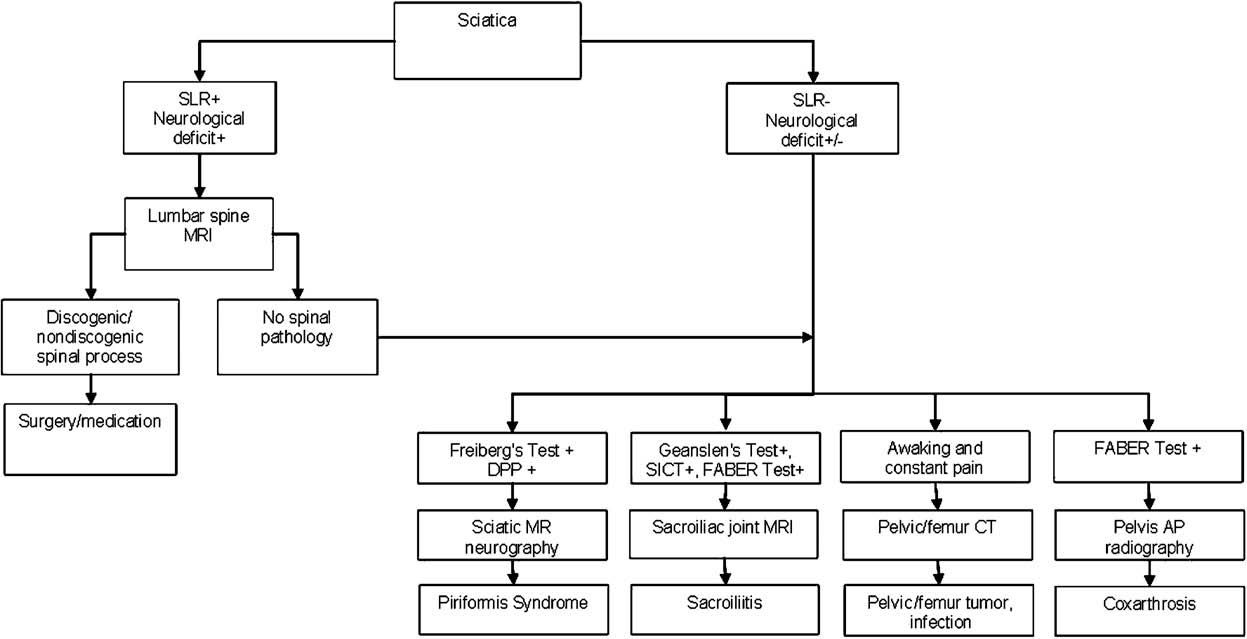
Fig. 7. An algorithm for the diagnosis of discogenic and non-discogenic sciatica. Sacroiliitis may cause posterior pelvic and sacroiliac pain during theFABER test, whereas coxarthrosis may cause groin pain during that test. In a few cases there is coincidence of spinal and extraspinal processes. In patientswhose spinal pathology has additional findings, extra examinations for extraspinal processes should be carried out. AP = anteroposterior radiography,DPP = deep piriformis palpation, SICT = sacroiliac compression test, SLR = straight leg raise test.
requires a careful and detailed physical and radiological
ever, may complicate the symptomatology, and require
examination based on a schema
careful evaluation.
3.1. Intraspinal causes of sciatica
3.2. Extraspinal causes of sciatica
Many intraspinal disorders can cause sciatica. There
Detection of extraspinal causes of sciatica is much more
may also be multiple processes, for instance intradural or
difficult than detection of intraspinal ones, and requires a
extradural cysts and tumors (mainly schwannomas), adult
high degree of caution. The main causes of extraspinal sci-
tethered cord syndrome, spinal epidural abscesses and
atica include sacroiliitis,intrapelvic processes,
hematomas, facet syndrome, lumbosacral deformities and
The pain pattern, and the presence or abscence of
3.3. Sacroiliitis and seronegative spondyloarthropathies
accompanying symptoms, are the most important compo-nents of the differential diagnosis.
Sacroiliitis, as one of the major causes of sciatica
The tumor-related pains commonly cause patients to
should be considered during the differential diagnosis
wake in the night. Whereas small schwannomas lead to
of LDHs, particularly when there is posterior thigh
radicular pain, larger tumors lead to accompanying
symptoms due to multiple nerve root and spinal cord
There are two potential mechanisms by which sacroiliitis
compressions. Epidural abscesses and hematomas may
can generate sciatica: (i) referred pain (e.g. patient 6), and
present with symptoms similar to intradural tumors.
(ii) direct involvement of the nerve by inflammatory medi-
Adult tethered cord syndrome may lead to sciatica asso-
ators released from the sacroiliac joint (e.g. patient 7).
ciated with a stretched thigh, resulting in gait distur-
Sacroiliitis is a common feature of seronegative spond-
bance. The pain of facet origin is located commonly in
yloarthropathies; the others include spondylitis, morning
the low back, buttock and thigh. It rarely extends to
stiffness, LBP, decreased mobility of the lumbar spine,
the lower levels. The pain secondary to deformities and
and peripheral arthritis.
instabilities is commonly associated with LBP and in-
The history of the patient and characteristics of the pain
creases in spine loading.
allow diagnosis of sacroiliitis and its etiology. The pain in
Fortunately, because lumbar MRI shows anatomical de-
sacroiliitis has an insidous onset, is commonly localized
tails of the lumbar spine, and other neural structures and
in the deep gluteal region and may refer to the posterior
soft tissues, making a diagnosis of spinal NDS is relatively
thigh. The pain decreases with activity and increases in
easy. Coincidental spinal and extraspinal disorders, how-
the late evening.
D.G. Kulcu, S. Naderi / Journal of Clinical Neuroscience 15 (2008) 1246–1252
The presence of LBP in patients with sacroiliitis makes
muscle tone not only produces local muscle pain but also
differential diagnosis complex. This is because LBP may
may result in sciatica.
indicate both ankylosing spondylitis and degenerative lum-
Patients with PS exhibit significantly different symptoms
bar spine. The patient needs to be questioned carefully to
and results of physical examination to those of patients
determine the symptoms that indicate the disease. Disc her-
with discogenic sciatica.Pain is the predominant symp-
niation-related LBP increases after activity and decreases
tom in both, but there are some differences in pain patterns.
after rest, whereas spondylitis-related LBP decreases after
There is usually sciatic notch tenderness or pain at the but-
activity, and increases during the latter half of the night.
tock in both patient groups. The pain of discogenic origin
Morning stiffness is another characteristic of spondylitis-
refers to the buttock and posterior thigh without any spe-
related LBP.
cific focal tenderness in the buttock. Unlike patients with
Physical examinations should include a Sacroiliac Com-
LDH, patients with PS typically experience symptoms in
pression Test, Gaenslen's test and a FABER test. The loca-
multiple dermatomes rather than either the lateral (S1
tion of the aggrevating pain after the FABER test may
radiculopathy) or the medial (L5 radiculopathy) derma-
reflect the pathology. Posterior pain in the pelvis may re-
tome alone. Numbness or weakness is quite uncommon
flect sacroiliitis, whereas pain in the groin may reflect
in PS. Unlike in LDH, the SLR test is generally negative
in patients with PS. Most patients with PS report that pro-
The early clinical diagnosis of sacroiliitis may be difficult
longed sitting and walking exacerbate their pain and that
and the diagnosis should be proven radiologically. Both CT
their symptoms reaggravate after internal rotation of the
and MRI are sensitive methods of demonstrating sacroiliitis.
The early CT scan findings include cortical erosions and sub-
The differential diagnosis of PS requires special tests
chondral sclerosis of the sacroiliac joints. The later CT scan
including Pace's sign, Freiberg's sign and deep digital pal-
findings include sacroiliac joint narrowing and ankylosi
pation of the piriformis muscle. If some of these tests are
MRI has a similar capacity to CT for detecting the disease;
positive, advanced radiological tests such as pelvic MRI
however, MRI can detect the early stages of sacroiliitis
and MRN should be performed since the pelvic MRI alone
because it can reveal bone marrow edema before morpho-
may fail to show the extraspinal parts of the sciatic nerve.
logic changes can be determined by a CT scan.
MRN may identify the sciatic nerve and its relationshipwith the surrounding structures.
3.4. Intrapelvic compressive processes
In one study, MRN had 93% specificity and 64% sensi-
tivity for distinguishing patients with PS from those with
Intrapelvic compressive processes may affect the nerve
similar symptoms by presenting piriformis muscle asymme-
as it passes from the neural foramina to the greater sciatic
try and sciatic nevre hyperintensity at the sciatic notch.
notch. Reported intrapelvic compressing processes include
Although piriformis muscle hypertrophy has been demon-
strated by MRI,Filler et al. also observed ipsilateral mus-
scesspresacral abscessand aneu
cle atrophy in some patieThis finding may be
Pelvic and femoral bone tumors may compress the sci-
secondary to disuse of the muscle in the chronic stage. In
atic nerve. Bickel et al. analyzed a surgical database of 32
the present study, MRN of patient 9 showed piriformis
patients with bone tumors that caused sciatica. According
muscle atrophy and asymmetry, and sciatic nerve hyperin-
to their analysis, the characteristics of the patient's pain
tensity. However, the MRI of patient 11 (who had PS),
are very important in the differential diagnosis of bone tu-
similar to Lee et showed that the piriformis muscle
mors. Sciatica due to bone tumors generally has an insi-
was not compressing the sciatic nerve. The absence of the
dous onset, causes constant pain, awakening at night,
positive finding in the neutral (static) position can be ex-
and is progressive and unresponsive to position changes.
plained by the dynamic nature of the piriformis muscle:
Local compression may reveal local tenderness. As most
as the pain is positive in Freiberg's position, MRI and
bone tumors occur in the pelvis or proximal femur, initial
MRN should be performed in both static and dynamic
pelvic radiography is recommended for patients with atyp-
positions (i.e. Freiberg's position).
ical sciatica. A simple pelvic radiograph may show tumor-related bony destruction, as in patient 8. Three-phase bone
3.6. Hip disorders
scintigraphy, CT scanning, and MRI seem to be sensitive indetecting bone tumors. MRI and MRN may show the rela-
The pattern of pain distribution in hip disorders may
tionship between the tumor and the sciatic nerve in detail.
create difficulty in determining the source of pain (spinevs. Swezey et al. reviewed patients who were treated
3.5. Piriformis syndrome
for lumbar spinal stenosis while the primary source of thepain was osteoarthrosis of the hip, and patients who were
Sciatica is caused by PS in 6% of patieHypertro-
treated for osteoarthrosis of the hip while the primary
phy, inflammation, anatomic variations, myositis ossificans
source of pain was lumbar spinal stenosis. Symptoms for
and traumatic injury of the piriformis muscle may com-
both disorders are frequently present in the same pa-
press the sciatic nerve.Any increase in the piriformis
tients.The presence of limb or groin pain, and limited
D.G. Kulcu, S. Naderi / Journal of Clinical Neuroscience 15 (2008) 1246–1252
internal rotation of the hips is predictive of a hip disorder
14. Naderi S, Manisali M, Acar F, et al. Factors affecting reduction in
rather than a spine disorder. The occurence of groin pain
during the FABER test may suggest a hip disorder. Pelvic
15. Chen WS. Chronic sciatica caused by tuberculous sacroiliitis. A case
radiography may show hip osteoarthritis.
report. Spine 1995;20:1194–6.
However, both hip and lumbar spine pathologies may
16. Parziale JR, Hudgins TH, Fishman LM. The PS. Am J Orthop.
exist together, as in patient 12. The radicular pain associ-
ated with progressive neurogenic claudication and neuro-
17. Brown MD, Gomez-Marin O, Brookfield KF, et al. Differential
diagnosis of hip disease versus spine disease. Clin Orthop Relat Res
procedure before a hip procedure.
18. Swezey RL. Overdiagnosed sciatica and stenosis, underdiagnosed hip
LDH is not the only cause of sciatica. A detailed patient
arthritis. Orthopedics 2003;26:173–4.
history, especially focused on pain characteristics, is an
19. van der Linden S, van der Heijde D. Ankylosing spondylitis. In: Haris
important component of patient evaluation. Physical
CB, Sledge CB, editors. Kelly's Textbook of Rheumatology. 6thed. Philadelphia: WB Saunders; 2001. p. 1039–53.
examination of patients with sciatica should include inspec-
20. Maksymowych WP, Landewe R. Imaging in ankylosing spondylitis.
tion, palpation, and all physical tests to exclude NDS.
Best Pract Res Clin Rheumatol 2006;20:507–19.
21. Battafarano DF, West SG, Rak KM, et al. Comparison of bone scan,
computed tomography and magnetic resonance imaging in thediagnosis of active sacroiliitis. Semin Arthritis Rheum 1993;23:161–76.
1. Bickels J, Kahanovitz N, Rubert CK, et al. Extraspinal bone and soft-
22. Geıjer M, Go¨thın GG, Go¨thın JH. The clinical utility of computed
tissue tumours as a cause of sciatica. Spine 1999;24:1611–6.
tomography compared to conventional radiography in diagnosing
2. Dudeney S, O'Farrell D, Bouchier-Hayes D, et al. Extraspinal causes
sacroiliitis. a retrospective study on 910 patients and literature review.
of sciatica: a case report. Spine 1998;23:494–6.
J Rheumatol 2007;34:1561–5.
3. Kralick F, Koenigsberg R. Sciatica in a patient with unusual
23. Odell RT, Key JA. Lumbar disc syndrome caused by malignant
peripheral nerve sheath tumors. Surg Neurol 2006;66:634–7.
tumors of bone. JAMA 1955;157:213–6.
4. Nishikawa T, Iguchi T, Honda H, et al. Primary bone tumors of the
24. Richardson RR, Hahn YS, Siqueria EB. Intraneural hematoma of the
femur presenting with spinal symptoms: a report of two cases and
sciatic nerve: case report. J Neurosurg 1978;49:298–300.
review of the literature. J Spinal Disord 2000;13:360–4.
25. Koga K, Osuga Y, Harada M, et al. Sciatic endometriosis diagnosed
5. Ortolan EG, Sola CA, Gruenberg MF, et al. Giant sacral schwan-
by computerized tomography-guided biopsy and CD10 immunohis-
noma. A case report. Spine 1996;21:522–6.
tochemical staining. Fertil Steril 2005;84:1508.
6. Wong M, Vijayanathan S, Kirkham B. Sacroiliitis presenting as
26. Andrews DW, Friedman NB, Heier L, et al. Tuboovarian abscess
sciatica. Rheumatology 2005;44:1323–4.
presenting as sciatic pain: case report. Neurosurgery 1987;21:100–3.
7. Yuksel KZ, Senoglu M, Yuksel M, et al. Brucellar spondylo-discitis
27. Macfarlane R, Pollard SG. Iliac and gluteal artery aneurysms
with rapidly progressive spinal epidural abscess presenting with
presenting as sciatica. J Roy Soc Med 1988;81:551–3.
sciatica. Spinal Cord 2006;44:805–8.
28. Aguilera V, Calvo F, Nos P, et al. Sciatica secondary to a presacral
8. Fishman LM, Zybert PA. Electrophysiologic evidence of pirı´formis
abscess as the first manifestation of Crohn's disease. Gastroenterol
syndrome. Arch Phys Med Rehabil 1992;73:359–64.
9. Jackson RP, Cain JE, Jacobs RR, et al. The neuroradiographic
29. Lewis AM, Layzer R, Engstrom JW, et al. Magnetic resonance
diagnosis of lumbar herniated nucleus pulposus: II. A comparison of
neurography in extraspinal sciatica. Arch Neurol 2006;63:1469–72.
computed tomography (CT), myelography, CT-myelography, and
30. Ozaki S, Hamabe T, Muro T. Piriformis syndrome resulting from an
magnetic resonance imaging. Spine 1989;14:1362–7.
anomalous relationship between the sciatic nerve and piriformis
10. Wiesel SW, Tsourmas N, Feffer HL, et al. A study of computer
muscle. Orthopedics 1999;22:771–2.
assisted tomography: I. The incidence of positive CAT scans in an
31. Filler AG, Haynes J, Jordan SE, et al. Sciatica of nondisc origin and
asymptomatic group of patients. Spine 1984;9:549–51.
piriformis syndrome: Diagnosis by magnetic resonance neurography
11. Akay KM, Ersahin Y, Cakir Y. Tethered cord syndrome in adults.
and interventional magnetic resonance imaging with outcome study of
Acta Neurochir (Wien) 2000;142:1111–5.
resulting treatment. J Neurosurg Spine 2005;2:99–115.
12. Naderi S, Aks
32. Jankiewicz JJ, Hennrikus WL, Houkom JA. The appearance of the
¨ , Men S, et al. Postoperative lumbosacral
instability: proposal of a new classification based on etiology. World
piriformis muscle syndrome in computed tomography and magnetic
Spine Journal 2007;2:16–21.
resonance imaging. A case report and review of the literature. Clin
13. Naderi S, Yucesoy K, Aks
Orthop Relat Res 1991;
¨ , et al. Epidural brucella abscess.
Report of a spinal brucellosis manifesting itself with epidural abscess.
33. Lee EY, Margherita AJ, Gierada DS, et al. MRI of PS. AJR Am J
Source: http://saitnaderi.com.tr/pdf/PDF70.pdf
Jansen et al. EJNMMI Research 2014, 4:8http://www.ejnmmires.com/content/4/1/8 18 F-FDG PET standard uptake values of thenormal pons in children: establishing a referencevalue for diffuse intrinsic pontine glioma Marc H A Jansen1*, Reina W Kloet2, Dannis G van Vuurden1,3, Sophie EM Veldhuijzen van Zanten1, Birgit I Witte4,Serge Goldman5, W Peter Vandertop6, Emile FI Comans2, Otto S Hoekstra2, Ronald Boellaard2and Gert-Jan JL Kaspers1
October 2010 Issue, Vol. 58 Table of Contents: News Province Wide Events & News in your Community Research Creative Solutions & Ideas Wheelchair Sports/Fitness Employment/Education Fund Development Classifieds Call for Submissions News – Province Wide Check out our Videos CPA (Alberta) has over 70 videos on our website, covering a wide variety of topics including housing, parenting, research, wheelchair transfers….and much more. Go to www.cpa-ab.org/odyssey List of Full Serve Gas Stations Go to www.cpa-ab.org/user_files/pdf/Gas_Stations_Full Service_April2010.pdf



