Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Untitled
IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 6, NOVEMBER 2012
WiiPD—Objective Home Assessment of Parkinson's
Disease Using the Nintendo Wii Remote
Jonathan Synnott
, Student Member, IEEE, Liming Chen
, Member, IEEE, Chris. D. Nugent
, Member, IEEE,
and George Moore
, Member, IEEE
Abstract—Current clinical methods for the assessment of
Reemergent postural tremor occurs when the user maintains a
Parkinson's disease (PD) suffer from inconvenience, infrequency,
fixed, unsupported position against gravity. Both of these forms
and subjectivity. WiiPD is an approach for the objective home-
of tremor involve oscillations at a frequency of 4–6 Hz. Kinetic
based assessment of PD which utilizes the intuitive and sensor-rich
tremor (also referred to as action tremor) may be the most de-
Nintendo Wii remote. Combined with an electronic patient diary,
bilitating form of tremor as it occurs during intentional limb
a suite of minigames, a metric analyzer, and a visualization en-
gine, we propose that this system can complement existing clinical
motion, such as during activity performance [3], yet this form
practice by providing objective metrics gathered frequently over
of tremor has received relatively little attention in research [4].
extended periods of time. In this paper, we detail the approach and
This form of tremor typically involves higher frequency oscil-
introduce a series of metrics deemed capable of quantifying the
lations occurring above 6 Hz [5]. In the earlier stages of PD,
severity of tremor and bradykinesia in those with PD. The system
tremor is typically presented unilaterally; however, as the dis-
has been tested on a 71-year-old participant with PD over a period
ease progresses symptoms may be presented bilaterally.
of 15 days, a 72-year-old control user without PD, and a group
of eight young adults. Results indicate a clear correlation between
Bradykinesia is defined as a reduction in speed of movement
patient self-rating scores of tremor severity and metric values ob-
during task performance. The term "bradykinesia" is often used
tained, in addition to clear differences in metrics obtained from
synonymously with two closely related symptoms: akinesia and
each user group. These results suggest that this approach is capa-
hypokinesia. Akinesia is described as a difficulty in initiating
ble of indicating the presence and severity of the motor symptoms
spontaneous movement, and is most commonly observed as
of PD that affect arm motor control.
freezing during walking [2]. Hypokinesia is poverty in move-
Index Terms—Motor assessment, Parkinson's disease (PD),
ment, expressed through reduced amplitude of movements such
as reduced arm swing during walking, or a reduced size ofhandwriting.
Rigidity is a resistance to passive movement which may occur
PARKINSON'S disease (PD) is a chronic neurodegenera- proximallyanddistally.Thismayappearina"cogwheel"form,
tive disease which is caused by the reduction in dopamine
where a ratchet sensation can be felt as resistance fluctuates
producing cells in the substantia-nigra region of the brain. This
during passive movement of a limb, or in a "lead-pipe" form
manifests itself as a series of debilitating motor and nonmotor
where rigidity is constant [6].
symptoms which can have a significant impact on activities of
Postural instability is indicative of advanced PD, and is a
daily living including dressing, washing, and eating. It is esti-
common cause of falls and injury [2].
mated that over 1150 000 people aged over 65 in Europe are
The National Institute for Health and Clinical Excellence
affected by PD, with an estimated cost of € 7577 (PPP) per
guidelines [7] recommend that patients with early stage PD who
are not yet undergoing medication should be assessed every 6–
The motor symptoms of PD appear in a variety of forms
12 months, and those who have begun treatment or who are ex-
including tremor, bradykinesia, rigidity, and postural instability.
periencing complications should be assessed every 2–3 months.
Tremor is an unintentional oscillating motion which is most
The Unified Parkinson's Disease Rating Scale (UPDRS) is one
noticeable in the distal regions of the body such as the arms,
of the most common clinical methods of PD assessment [8].
legs, and jaw [2] and can appear in a number of forms. Rest-
This scale assesses 42 aspects of PD, split into four categories:
ing tremor, the most common form of tremor associated with
mentation, behavior, and mood; activities of daily living; mo-
PD, occurs when the affected region of the body is at rest and
tor issues; and complications of therapy. Each aspect is rated
subsides during the onset of movement of the affected limb.
on a five-point scale where 0 represents no impairment due toPD, and 4 represents severe impairment. Assessment relies ona combination of motor examinations performed by a trained
Manuscript received November 29, 2011; revised May 12, 2012; accepted
August 21, 2012. Date of publication August 28, 2012; date of current version
clinician and patient recall of the prevalence and characteristics
November 16, 2012. This work was supported in part by the Healthcare Infor-
of certain symptoms since the previous assessment.
matics Society of the Ireland Research Bursary and in part by the Department
This method of assessment is subjective and is, therefore, ex-
of Employment and Learning, Northern Ireland.
posed to issues with accuracy and consistency of results. These
The authors are with the Computer Science Research Institute and the
School of Computing and Mathematics, University of Ulster, Jordanstown, Co.
assessments typically require travel to a clinic which may be in-
Antrim BT37 0QB, N. Ireland, U.K. (e-mail:
[email protected];
convenient especially to those with advanced motor disability.
Stress and anxiety, which is said to negatively affect symp-
Color versions of one or more of the figures in this paper are available online
toms [9], may be present during such assessments and results
Digital Object Identifier 10.1109/TITB.2012.2215878
obtained may, therefore, not provide an accurate representation
1089-7771/$31.00 2012 IEEE
SYNNOTT
et al.: WIIPD—OBJECTIVE HOME ASSESSMENT OF PARKINSON'S DISEASE USING THE NINTENDO WII REMOTE
of the typical severity of symptoms. Additionally, these assess-
tremor and bradykinesia values between PD users on medica-
ments only provide a snapshot of the condition at the time of
tion, off medication, and control users.
assessment and are unable to capture the fluctuations under a
Accelerometers suffer from the need for specific placement
condition that may occur on an hourly or daily basis.
and orientation on the body to ensure reliability and consistency
There is, therefore, the potential for sensor-based approaches
of results [14]. This may not be ideally suited for long-term
to complement existing clinical assessment techniques, offering
unsupervised assessment of nontechnical users. To address this
advantages in terms of objectivity, consistency, and frequency of
issue, Niazmand
et al. [15] introduced a smart garment consist-
data collection. When deployed in the home environment, such
ing of eight integrated accelerometers worn on the upper body.
solutions can facilitate more frequent and convenient assess-
This garment was able to correctly identify rest tremor (sensitiv-
ment, providing more detailed information about the fluctuation
ity 71%) and postural tremor (sensitivity 89%), but also required
of symptoms throughout the day. Ultimately, this can allow
users to perform specific UPDRS motor tasks to facilitate de-
clinicians to make more informed decisions about treatment
adjustment, maximizing patient quality of life.
Computer vision-based approaches incorporate the use of
Various studies have been undertaken which investigate the
camera technology to facilitate the tracking of objects within an
use of portable sensor technology to quantify the severity of PD
environment, offering the advantage of unobtrusiveness which
motor symptoms. These studies use a range of approaches in-
may be particularly advantageous for long-term assessment.
cluding the use of accelerometers, computer vision, traditional
Synnott
et al. [16] proposed an approach to motor assessment
PC peripherals, and bespoke hardware. However, there is typi-
using passive markers attached to objects involved in activities
cally a tradeoff between obtrusiveness, ease of use, richness of
of daily living. This study highlighted the ability for such an
data, and hardware expense. The goal of WiiPD is to expand on
approach to differentiate between normal and abnormal motor
existing research by applying the Nintendo Wii remote (NWR)
performance, quantifying the amplitude of tremor present while
device to long-term at-home PD assessment. Initial control user
participants drank from a cup. Starner
et al. [17] introduced
testing as detailed by Synnott
et al. [10] indicated the potential
the gesture pendant, a wearable camera-based device capable
of such an approach in differentiating between normal and ab-
of recognizing hand gestures and identifying the frequency of
normal user behavior. The NWR, which offers an ideal balance
tremor present during hand movement. While the unobtrusive
between ease of use, richness of data, and expense, is used to
nature of computer vision approaches may increase compliance
interact with a software system designed to capture the severity
over extended periods of monitoring, these approaches suffer
of PD motor symptoms. This software incorporates a series of
from data inconsistency due to marker occlusion.
bespoke motor tasks presented in the form of minigames which
Various studies have utilized dedicated hardware devices
are designed to capture PD motor symptoms, coupled with a
for the objective home assessment of PD. Goetz
et al. [18]
metric analyzer which provides objective metrics detailing user
developed a bespoke computer-based at-home testing device
performance. Additionally, the approach offers an electronic pa-
equipped with a range of tests including button tapping, peg-
tient diary to record medication intake information and symptom
board plugging, wrist acceleration, and speech. Patient UPDRS
self-ratings, as well as a visualization engine which is capable
scores declined during the study, best indicated by finger tap-
of providing a visual overview of user performance to aid the
ping, tremor, and speech tests. This study highlighted the feasi-
understanding of gathered metrics.
bility of home-based assessment of PD through high complianceand satisfaction rates. Westin
et al. [19] introduced a portabletesting tool consisting of a series of diary questions and mo-
II. RELATED RESEARCH
tor tasks presented on a PDA device. The study had a median
Previous studies into the use of sensor-based approaches for
compliance of 93% and found that the speed of performance in
the analysis of PD motor symptoms have incorporated a wide
uncued alternate target tapping and random target tapping tasks
range of sensor technology.
was higher in participants recorded to be in an "on" medica-
One popular approach involves the use of accelerometers
tion state. Keates and Trewin [20] developed a target clicking
or gyroscopes attached to various points on the body. Patel
exercise to be completed using the mouse, facilitating the anal-
et al. [11] investigated the use of eight accelerometers placed on
ysis of cursor velocity and pauses during movement. This study
the arms and legs to predict clinical scores of tremor, bradyki-
identified lower mean peak velocities in users with PD. Cun-
nesia, and dyskinesia during UPDRS motor task performances.
ningham
et al. [21], [22] developed a similar tool incorporating
Average estimation errors of tremor, bradykinesia, and dyskine-
a point and click exercise to be completed using the mouse,
sia were 3.4%, 2.2%, and 3.2%, respectively. Giuffrida
et al. [12]
and found significant differences in cursor movement speeds
introduced an approach involving a portable device worn on the
and task completion times not only between PD and non-PD
wrist and finger, containing three orthogonal accelerometers and
users, but also between PD users who were in "on" and "off"
gyroscopes. While participants performed UPDRS motor tasks,
medication states. However, significant differences in median
the system was found to be capable of evaluating rest, postural,
completion times between experienced and inexperienced com-
and kinetic tremor producing a high correlation with clinical
puter users with PD suggest that a more intuitive input device
UPDRS scores (highest
r2 = 0.89, 0.90, and 0.69 respectively).
may be advantageous for such assessments.
Salarian
et al. [13] studied the use of 3-D gyroscopes attached
We present an approach which extends existing research into
to the wrist in order to quantify tremor and bradykinesia while
the long-term home-based assessment of PD. This approach fa-
participants performed a range of activities of daily living. This
cilitates the assessment of motor and nonmotor symptoms of PD
approach was capable of detecting significant differences in
through the use of the NWR combined with bespoke software.
IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 6, NOVEMBER 2012
display. This camera, with a resolution of 1024 × 768 pixels,a 100 Hz sample rate, and a 45◦ field of view, provides datadescribing the NWR's position and orientation in relation to thesensor bar, allowing it to be used as an accurate pointing devicefor on-screen cursor control. Finally, 12 binary input buttonsplaced at various locations on the body of the NWR facilitatedirect input by the user.
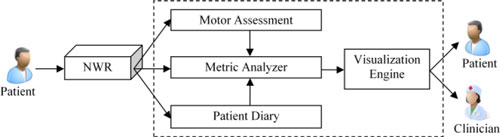
WiiPD system architecture presenting the link between the main com-
ponents within the system.
B. Motor Assessment
This device is designed to be intuitive to use and may, there-
The motor assessment component of the architecture is de-
fore, provide advantages over dedicated accelerometer devices
signed to capture various elements of PD motor dysfunction by
in terms of the accuracy and consistency of data collected in
requiring the user to complete a series of software-based motor
addition to increasing user compliance over extended periods of
tasks using the NWR.
use. Additionally, this sensor-rich device may offer more rich
As this study incorporates the use of a handheld device by
data about PD motor symptoms than traditional input devices or
a single user to facilitate motor analysis, it was decided that
computer vision systems. The incorporation of a series of motor
the focus of the study would be the motor symptoms of PD
tasks presented in the form of minigames can replace the need
which primarily affect arm and hand motor control. For this
for supervision or training in the performance of UPDRS motor
reason, tremor and bradykinesia were chosen to be the primary
tasks while maximizing the consistency of performance.
symptoms to be captured and quantified.
The motor tasks are presented in a minigame format which
have the potential to provide a number of benefits over tra-
The architecture of the approach comprises several compo-
ditional formats of unsupervised clinical or rehabilitative [26]
nents. The relationship between each of these components is
unsupervised long-term home-based exercise. Minigames con-
highlighted in Fig. 1.
sist of short duration, goal-oriented tasks with clear objectives,
The following section describes each of these architectural
facilitating casual usage with minimal training and setup time.
components in further detail.
Minigames can be designed to constrain user movement whilerewarding correct performance. This has the potential to re-duce the occurrence of incorrect movement actions which may
A. Data Collection (NWR)
become more prevalent over extended periods of time, espe-
As PD most commonly affects those who are over the age of
cially if the user finds a certain movement difficult. A reduction
50, careful consideration about the method of input is required.
in monotony can be achieved by designing minigames to be
Users of this age group tend to interact with computers less
fun and engaging, with the goal of increasing user compliance
often [23], and as a result may be less familiar with traditional
throughout extended monitoring periods and reducing the stress
input devices such as the keyboard and mouse. Further difficul-
and anxiety present during patient clinical assessment.
ties with the use of such devices may arise due to the symptoms
Many minigames are currently available for the Nintendo
of PD and other cognitive or physical conditions which are
Wii; however, it was decided that a bespoke solution would be
more commonplace in the aging population. Additionally, such
developed. This facilitates optimization of tasks to best capture
traditional input devices are typically not designed to facilitate
the various aspects of PD motor dysfunction, ensuring consis-
motion analysis and are, therefore, unable to fully capture the di-
tency and complete control over the demands placed on the
verse range of components associated with PD motor symptoms.
user. PD motor symptoms are dynamic and often situational.
Nontraditional input methods such as dedicated accelerometer
For example, the postural, kinetic, and rest elements of tremor
devices are suited for capturing motor performance metrics;
only appear under certain conditions. As a result, a series of
however, these typically require specific placement and orien-
minigames were designed to invoke these conditions. These
tation in order to ensure reliability and consistency of results.
minigames incorporate randomization where possible in order
This added complexity may render such devices unsuitable for
to minimize the effect of task learning. The minigames devel-
longer term usage without regular supervision.
oped were target shooting, target holding, and target following.
The ideal device for unsupervised monitoring over extended
These tasks each primarily make use of the IR camera for
periods of time must be robust, intuitive to use, and capable
interaction. By pointing the NWR at a sensor bar positioned
of capturing the various aspects of PD motor dysfunction. The
below the screen, the user is required to move an on-screen
NWR meets these requirements, and has been chosen as the
cursor in response to the appearance of visual targets. The target
primary input device for the system. The NWR is a wireless,
shooting task requires the user to press the trigger button while
handheld device which contains a range of sensor technology
holding the cursor over a series of randomly positioned targets
for data collection, as detailed in [24]. An onboard ADXL 330
and is complete once 20 targets have been selected. This task has
accelerometer [25] is capable of capturing acceleration along
been designed to highlight the presence of any kinetic tremor and
three axes with a range of ± 3g at a sample rate of up to 100 Hz.
bradykinesia by combining elements of gross motor movement
Additionally, an onboard PixArt Imaging infrared camera is
(between each target) and fine motor control (the selection of
located at the front of the device, designed to be used with
each target). The target holding task is similar to the target
an infrared light emitting sensor bar placed above or below a
shooting task as the user must move the cursor over a series of
SYNNOTT et al.: WIIPD—OBJECTIVE HOME ASSESSMENT OF PARKINSON'S DISEASE USING THE NINTENDO WII REMOTE
which are proposed to indicate the severity of various PD motor
PARTICIPANT SELF-ASSESSMENT SCALE
symptoms. The metrics are as follows.
Unfiltered cursor movement speed, UMS (pixels/second),
describes the raw cursor movement speed including the low-frequency gross motor movements required for task comple-tion and the high-frequency fine motor movements indicativeof tremor. This value is determined by calculating the meanEuclidean distance traveled by the cursor per second. This ap-proach is detailed in (1), in which n = the number of datasamples recorded for one task, i = the index of the current datapoint, X and Y = the X and Y coordinates of the cursor insample i, and Timestamp = the time (in seconds) that sample iwas recorded:
randomly positioned targets. In this task, however, the user must
i − Xi−1 )2 + (Yi − Yi−1 )2
maintain a cursor position over the target for 10 s. This task has
Timestamp − Timestamp
been designed to highlight the presence of postural tremor by
Filtered cursor movement speed, FMS (pixels/second), de-
requiring the user to maintain a fixed cursor position for a set
scribes the cursor movement speed after it has been processed
period of time. In the target following task, the user must track
through a moving average filter. This filter removes the com-
the movements of one target with the cursor for 30 s. In this
ponents of high frequency oscillation caused by tremor while
task, the target moves along a random path at a fixed speed. The
preserving the lower frequency gross motor movements required
purpose of this task is to assess the user's ability to complete
for task completion. Extensive testing revealed a moving aver-
constrained fine motor movements, highlighting the presence of
age sample size (w) of 11 to best isolate PD tremor components.
kinetic tremor or bradykinesia.
As cursor movement using the NWR is subject to interruptiondue to IR bar occlusions and interference, any moving average
C. Patient Diary
window periods that contain samples recorded during IR bar
The patient diary component of the architecture was designed
occlusion are omitted. UMS and FMS may be calculated during
to provide supporting information about the user which cannot
target intersection (when the cursor is held over the target) and
be captured through interaction with the motor assessment tasks.
during periods of nonintersection (when the cursor is moving
The two areas of information captured relate to medication in-
between targets).
take and self-perceived severity of symptoms. The user is asked
Residual magnitude, RM (pixels), describes the mean Euclid-
to enter the type of medication last taken (patch or pill), along
ian distance between the filtered (FX, FY) and unfiltered (X, Y )
with the time of the last dosage. Additionally, the user is in-
movement coordinates, providing an indication of the amplitude
structed to provide a subjective assessment of the self-perceived
of tremor present during task performance. This is described in
severity of motor symptoms at the time of interaction with the
(2), in which n = the total number of data samples for a task
performance, i = the current sample index, and w = the moving
As patients have been shown to have trouble distinguishing
average window size:
between medication states and identifying the presence of medi-
cation complications even after training [27], it was decided that
(F Xi − X w +i)2 + (F Yi − Y w +i)2.
a simple five-point scale would be used for patients to record
their perceived severity of symptoms. Rather than being asked toclassify their current state, this scale requires users to intuitively
Target intersect %, TI, describes the total percentage of time
compare the current severity of symptoms to that of a typical
a user was able to maintain a cursor position on a moving target,
day. This scale is adapted from the Parkinson's self-assessment
providing an indication of the impact of bradykinesia and tremor
tool [28] which was developed by the cure Parkinson's trust
on a user's ability to track a moving target.
and is supported by Parkinson's UK [29]. Table I provides a
Click accuracy, CA (% correct clicks), provides an indication
full description of the scale. When recording the presence of
of the impact of PD motor symptoms on the completion of
any symptoms, users are asked to name the symptom, describe
fine motor tasks. This is calculated by comparing the number
which area of the body is affected, and provide a rating, for
of correct clicks to the number of incorrect clicks (see (3)). A
example, tremor, right hand, 2.
correct click is defined as a button press performed while thecursor intersects with the desired target. An incorrect click isdefined as any other unnecessary button press:
D. Metric Analysis
Total Clicks − Total Incorrect Clicks
The metric analyzer processes data from the NWR, the mo-
× 100.
tor assessment tasks, and the patient diary component. Data
gathered from each interaction session are stored in comma
Completion time, CT (milliseconds), describes the total time
separated variable files and can be individually processed on
taken to complete tasks which are not time limited. Calculation
a session-by-session basis or batch processed for trend analy-
of CT was adapted to take into account the possibility of IR bar
sis. The data samples are analyzed to derive a series of metrics
occlusion and IR interference which prevents task progression.
IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 6, NOVEMBER 2012
the current states of various game components are recorded,
MOTOR TASK OVERVIEW
facilitating visual reconstruction of task completion. As the IRcamera is susceptible to marker occlusion and interference fromother IR sources, robust filtering techniques were required tomaximize the accuracy of the metrics obtained.
A. Study Protocol
Our test cohort consisted of three user types: an older adult
with PD (PDP), an older adult of similar age without PD (OA),and a younger adult group (YAG) consisting of eight controlparticipants with no formally diagnosed motor conditions. In-formed consent was received from all volunteers in accordancewith the University of Ulster's Research Ethics Committeeguidelines and approval.
The PDP was a right-handed 71-year-old male who had been
diagnosed with PD for 6 years at the time of involvement. Thisparticipant recorded two sessions per day for 15 days. During
Periods of IR bar occlusion are detected and subtracted from the
the study, his medication intake consisted of two 8 mg Neupro
transdermal patches per day in addition to four Sinemet Plus
Target re-entries count, TRC, describes the number of times
tablets per day during the first week of the study, and three
the cursor leaves and reenters the target after the first entry,
per day during the second week of the study. His symptoms
providing an indication of the impact of tremor on a user's
included a marked rest and postural tremor of variable severity
ability to maintain a fixed position.
on the right hand which subsides during action. The participant
The relationship between the motor tasks, metrics, and PD
reported that this tremor was not immediately apparent upon
symptoms is presented in Table II.
waking up. This participant had previous experience with theuse of the NWR for interaction with off-the-shelf Nintendo Wii
E. Visualization Engine
games. This participant's involvement was largely unsupervised.
The visualization engine is designed to consolidate and visu-
The participant was provided with user documentation which
alize gathered metrics in a manner which best aids the under-
detailed the setup and usage procedures, and weekly phone calls
standing of the collected data. For this study, we have developed
were arranged in order to discuss any issues. As this participant
a technique that provides benefits for long-term at-home assess-
displayed a tremor with a significant range of severities, it was
ment. This technique involves fine-grained visual reconstruction
decided to evaluate the system on this single PD participant over
of individual task performance, displaying previous user inter-
an extended period of time as an alternative to evaluating many
action with the system in a summary (showing all details of the
users for shorter time periods. This provides a dataset capturing
entire performance at once) or real-time format. This involves
a range of symptom severities, facilitating the evaluation of the
displaying the cursor movement path and game objects, allow-
system's potential for quantification of symptom severity.
ing clinicians to view the visible signs of motor symptoms such
The OA was a right-handed 72-year-old male who suffered
as tremor or bradykinesia. These visual reconstructions facilitate
from arthritis in his right hand. This participant owned a Nin-
verification of user self-rating scores, and aid the identification
tendo Wii and had previous experience with the use of the NWR
and resolution of usability issues such as user error or hardware
for game interaction. This participant's involvement was super-
issues such as IR bar occlusion and interference. This unobtru-
vised, and the equipment was set up for him in his home.
sive method of monitoring user interaction is of particular use
The YAG consisted of eight members of university staff and
during long-term unsupervised home assessment periods and
students (seven males and one female) with a mean age of 28
facilitates remote monitoring of user performance without the
(SD = 3.7). Participants in this group ranged from having little
need for a home visit.
or no experience with the NWR, to having regular experience
Examples of this visualization technique can be seen in Fig. 2.
of weekly use. These participants were supervised and had theequipment set up for them. The OA and YAG control users wereincluded in this study to provide a baseline set of data samples
IV. IMPLEMENTATION AND TESTING
that are unaffected by the symptoms of PD.
WiiPD was implemented in C# using the XNA Framework
Each participant was supplied with a Brite Computers Class-
v3.1. Data collection from the NWR was facilitated using the
mate PC [31] with the WiiPD software preinstalled, a wireless
WiimoteLib library v1.7 [30] which provides access to the data
IR bar, an NWR, and a Bluetooth dongle. Participants were also
generated by each of the NWR's sensors. The sensor data were
supplied with a user guide that detailed hardware setup and us-
sampled at a rate of 46 Hz, providing a Nyquist frequency suffi-
age, the study protocol, and an explanation of the correct posture
cient to capture the frequency ranges associated with PD tremor.
to maintain during recording.
Each data sample contains a description of the current state of
Each recording session involved the user completing each
the NWR and its sensors, facilitating postprocessing of the raw
task in series with their right hand, followed by their left hand.
data for metric analysis. In addition to the NWR sensor data,
On-screen prompts were used to introduce each task, reminding
SYNNOTT et al.: WIIPD—OBJECTIVE HOME ASSESSMENT OF PARKINSON'S DISEASE USING THE NINTENDO WII REMOTE
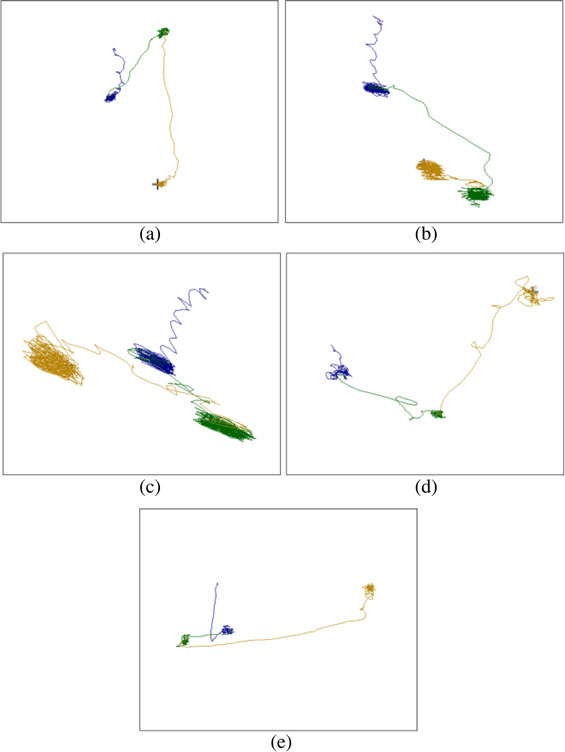
Example movement paths showing completion of T1 with PDP: (a) SR = 1, (b) SR = 2, (c) SR = 3, (d) a typical OA performance, and (e) typical YAG
the user about the steps required to complete the task and show-
miliarize themselves with the system before recording sessions
ing the user visually how the NWR should be held. Participants
were instructed to maintain a specific posture during all record-ing sessions. This posture required the participant to sit uprightin a chair, with the elbow of the active arm at rest on the arm
V. RESULTS AND DISCUSSION
of the chair, leaving the forearm free of obstruction and mini-
The Appendix contains an overview of the results obtained
mizing postural fatigue. Initial testing revealed that adjustment
from left- and right-hand task performances by each of the
of the distance between the NWR and IR bar impacted cursor
participant groups. Results obtained from the PDP have been
movement sensitivity. It was found that cursor movement sensi-
divided by tremor self-rating (SR). The PDP provided self-
tivity decreased as distance from the IR bar increased. Although
ratings for 100% of the recording sessions. All of the self-ratings
this change in sensitivity was not significant, users were asked
described a right-hand tremor, with 4 sessions receiving a self-
to maintain a consistent distance from the IR bar during all
rating of 1 (better than usual), 22 sessions receiving a rating of
recording sessions.
2 (typical), and 4 sessions receiving a self-rating of 3 (worse
The PDP was asked to complete recording sessions with the
than usual). SR scores were used as a benchmark to validate
system at four time periods: immediately before the first medica-
the ability of the tasks and metrics to differentiate between
tion intake of the day (AM-B ), 30 min after the first medication
tremor severities. A blind evaluation was performed in order
intake of the day (AM-A), immediately before the last med-
to determine the reliability of the participant self-ratings. This
ication intake of the day (PM-B ), and 30 min after the last
evaluation involved manually assessing each performance of
medication intake of the day (PM-A). The OA was asked to
each task and assigning a predicted self-rating score based on
complete recording sessions during midmorning and midafter-
the amplitude of tremor, the prevalence of tremor throughout the
noon. In total, 30 sessions were recorded by the PDP, 6 sessions
task, and the impact of the tremor on task completion. The visual
were recorded by the OA, and each of 8 YAG participants were
reconstruction of cursor movements was used to facilitate this.
recorded once. All participants were given the opportunity to fa-
The assessor was unaware of the self-rating scores assigned by
IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 6, NOVEMBER 2012
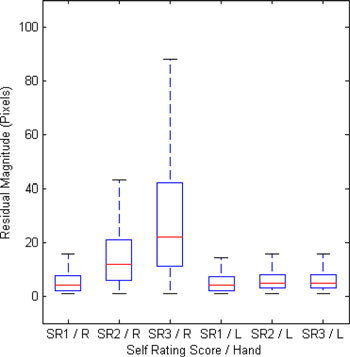
Box plots displaying the relationship between PDP SR scores for right-
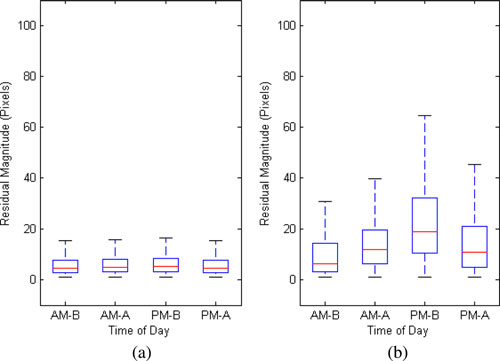
Box plots displaying the relationship between time of day and the
hand tremor severity (higher score = more severe) and the distribution of RMs
distribution of RMs recorded during completion of T1, T2 and T3 with (a) left
recorded during completion of T1, T2 and T3 excluding outliers.
hand and (b) right hand excluding outliers. AM-B = AM - before medication;AM-A = AM - after medication; PM - B = PM - before medication; PM-A =PM - after medication.
the participant, and each task was evaluated independently, i.e.,when assigning a score to one task, the assessor was unaware ofthe score they had assigned to the other tasks in the same session.
The results from the evaluation of a total of 90 task performancesproduced a correct prediction percentage of 72.2%.
This section provides an overview of all results obtained,
offering detailed discussion on metrics which show a significantdifference (p< 0.05) between right-hand performances groupedby SR. Significance of results was determined by performingKruskal–Wallis tests on the mean values of metrics for each taskperformance.
A. Cursor Movement Paths
Fig. 2 provides an example of movement traces from T1 (tar-
get holding) performances with the right hand by the PDP witheach self-rating score, one example of a typical OA performance,and a typical YAG performance. In these examples, the pointat which the user maintained a fixed position over each of the
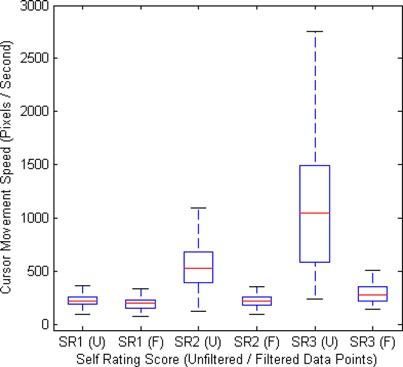
Box plots highlighting the relationship between self-rating scores and
filtered/unfiltered cursor movement speeds obtained during right-hand perfor-
three targets for 10 s can be identified by distinct areas of more
mances of T2 by the PDP excluding outliers (F = filtered movement speed; U
densely grouped movement traces. SR1 performances can be
= unfiltered movement speed).
seen to resemble those by the OA and YAG, and the movementtrace groupings during target holding can be seen to increasewith size as SR increases. Additionally, the movement paths
raw cursor movement and cursor movement passed through a
between each target show larger oscillations as SR increases.
moving average filter is capable of indicating the presence and
This pattern was consistent for T1, T2, and T3.
amplitude of the fine motor movements associated with tremor.
The PDP RM values obtained during performances of T1,
T2, and T3 grouped by time period are highlighted in Fig. 4.
B. Residual Magnitude
There is a significant difference between the right-hand RMs
The PDP RM values obtained for each performance of T1,
gathered throughout the day (p = < 0.001), and no significant
T2, and T3 grouped by SR are summarized in Fig. 3. There is a
difference in the left hand RMs gathered throughout the day (p
significant difference (p < 0.001) between the self-rating groups
= 0.8835). In regards to right-hand performance, the highest
recorded with the tremor affected right hand and no significant
median (18.87 pixels) and IQR (21.62 pixels) are observed in
difference (p = 0.7975) between those recorded with the unaf-
the PM-B time period, whereas the lowest median (6.40 pixels)
fected left hand. A clear relationship can be observed between
and IQR (11.16 pixels) are observed in the AM-B medication
the self-rating score and the RM distribution for recordings with
time period. There is a significant difference (p = < 0.001) in
the right hand. It can be seen that as tremor SR increases, the me-
residuals recorded just before medication intake (AM-B, PM-
dian RM and IQR of magnitudes increase. All left-hand record-
B) whereas the residuals recorded just after medication intake
ings have a consistently low median RM and IQR. This indicates
(AM-A, PM-A) show more similarity and are not significantly
that the calculation of RM by calculating the difference between
different (p = 0.7848). Interestingly, residuals recorded in the
SYNNOTT et al.: WIIPD—OBJECTIVE HOME ASSESSMENT OF PARKINSON'S DISEASE USING THE NINTENDO WII REMOTE
medicated AM-A time period tend to be significantly higher (p
Interestingly, both the LH and RH CA values were consistently
= 0.0274) than those recorded in the nonmedicated AM-B time
lower for the PDP compared to the OA and YAG.
period. These results support PDP SR trends, in which AM-Brecordings typically received lower SR ratings (AM-B SR1 =
E. System Usability
37.5%, SR2 = 62.5%, SR3 = 0%), whereas PM-B recordings
In order to determine the feasibility of the NWR to be used
typically received higher SR ratings (PM-B SR1 = 0%, SR2
as an input device for long-term unsupervised monitoring, we
= 71.4%, SR3 = 28.6%). These results also support the PDP's
assessed the prevalence of the primary source of input error. Dur-
own observations that tremor worsens throughout the day.
ing testing and evaluation, it was observed that IR bar occlusionand IR interference were the primary sources of data collection
C. Movement Speeds
interruption. The median percentages of samples excluded fromanalysis due to IR occlusion were as follows: PDP 0.28%; OA
Fig. 5 provides an overview of the UMS and FMS values
0.92%; YAG 0%, indicating that these events are relatively rare
obtained during performances of T2 grouped by SR. It can be
and the effects of which can be minimized through exclusion
observed that as tremor SR increases, mean unfiltered movement
of affected data samples during data analysis combined with
speeds increase significantly (p = 0.0051). Filtered movement
robust filtering techniques.
speeds show a small increase; however, the difference is notsignificant (p = 0.0666). As tremor severity increases, the dif-ference between UMS and FMS also increases. These results
VI. CONCLUSION AND FUTURE WORK
indicate that the moving average technique is capable of iso-lating the gross motor movements required for task completion
This paperhas introduced WiiPD, an approach to the objective
from the high-frequency, high-velocity tremor components.
home assessment of PD using the NWR. The main componentsof WiiPD have been detailed, including a range of motor tasks,a metric analyzer, a patient diary system, and a visualization en-
D. Task Completion Metrics
gine. The system has been tested on a participant with PD who
TRE, TI, and CA were proposed to indicate the impact of PD
experiences a right-hand tremor of varying severity, a similarly
symptoms on completion of tasks which involve cursor move-
aged control user, and a group of eight healthy young adults. A
ment. It was found that as SR increased, PDP RH TRE counts
strong correlation was found between participant self-ratings of
increased significantly (p = 0.0034), indicating that tremor had
tremor severity and the metrics collected during motor task per-
a significant impact on the PDP's ability to maintain a fixed
formance. In particular, cursor movement speed and RMs were
cursor position over a target.
shown to be key indicators of the presence and severity of tremor.
The PDP's RH TI percentages were consistently lower than
Future work will include a larger study involving a larger number
those recorded by the OA and YAG. The TI percentages were
of participants with a range of symptoms at various severities.
found to decrease as SR increased; however, the difference be-
This will facilitate the assessment of the impact of multiple
tween SR groups was not significant (p = 0.069).
symptoms affecting motor performance simultaneously. This
The PDP's RH CA values decreased significantly (p =
study will consist of system usage over a period of several
0.0496) as SR increased, indicating that tremor has a significant
months, coupled with UPDRS assessments to assess the ability
impact on the PDP's ability to click on-screen targets accurately.
of the system to detect subtle changes in condition over time.
IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 6, NOVEMBER 2012
[21] L. Cunningham, C. Nugent, G. Moore, D. Finlay, S. Mason, and D. Craig,
"Home-based monitoring and assessment of Parkinson' s disease," IEEE
The authors would like to thank the volunteers who kindly
Trans. Inf. Technol. Biomed., vol. 15, no. 1, pp. 47–53, Jan. 2011.
offered their time, support, and feedback throughout the study.
[22] L. M. Cunningham, C. D. Nugent, G. Moore, D. D. Finlay, and D. Craig,
"Computer-based assessment of movement difficulties in Parkinson'sdisease," Comput. Methods Biomech. Biomed. Eng., pp. 1–12, May2011. [Online]. Available: http://www.tandfonline.com/doi/abs/10.1080/
[23] D. P. Lorence and H. Park, "New technology and old habits: The role of
[1] P. Andlin-Sobocki, B. J¨onsson, H. U. Wittchen, and J. Olesen, "Cost of
age as a technology chasm," Technol. Health Care, vol. 14, pp. 91–96,
disorders of the brain in Europe," Eur. J. Neurol., vol. 12, pp. 1–27, 2005.
[2] J. Jankovic, "Parkinson's disease: Clinical features and diagnosis," J. Neu-
[24] J. C. Lee, "Hacking the Nintendo wii remote," IEEE Pervasive Comput.,
rol. Neurosurg. Psychiatry, vol. 79, pp. 368–376, 2008.
vol. 7, no. 3, pp. 39–45, Jul./Sep. 2008.
[3] J. Raethjen, S. Pohle, R. Govindan, A. Morsnowski, R. Wenzelburger,
[25] Analog Devices, (2011, Sep. 20). Small, low power, 3-axis ± 3 g
and G. Deuschl, "Parkinsonian action tremor: Interference with object
� Accelerometer [Online]. Available: http://www.analog.com/
manipulation and lacking levodopa response," Exp. Neurol., vol. 194,
pp. 151–160, 2005.
[26] J. Decker, H. Li, D. Losowyj, and V. Prakash, "Wiihabilitation: Rehabil-
[4] P. Kraus, M. Lemke, and H. Reichmann, "Kinetic tremor in Parkinson's
itation of wrist flexion and extension using a wiimote-based game sys-
disease—An underrated symptom," J. Neural Trans., vol. 113, pp. 845–
tem," Governor's School Eng. Technol. Res. J., 2009. [Online]. Available:
[5] R. Wenzelburger, J. Raethjen, K. L¨offler, H. Stolze, M. Illert, and
[27] C. G. Goetz, S. Leurgans, V. K. Hinson, L. M. Blasucci, J. Zimmerman,
G. Deuschl, "Kinetic tremor in a reach-to-grasp movement in Parkinson's
W. Fan, T. Nguyen, and A. Hsu, "Evaluating Parkinson's disease patients
disease," Movement Disorders, vol. 15, pp. 1084–1094, 2000.
at home: Utility of self-videotaping for objective motor, dyskinesia, and
[6] D. Weintraub, C. L. Comella, and S. Horn, "Parkinson's disease: Part 1.
ON–OFF assessments," Movement Disorders, vol. 23, pp. 1479–1482,
Pathophysiology, symptoms, burden, diagnosis, and assessment," Amer.
J. Manag. Care, vol. 14, pp. S40–S48, 2008.
[28] The Cure Parkinson's Trust. (2011, Oct. 14). Parkinson's self assessment
[7] National Institute for Health and Clinical Excellence. (2006). Parkin-
son's disease: Diagnosis and management in primary and secondary
care. Royal College of Physicians. London, U.K. [Online]. Available:
[29] Parkinson's UK. (2011, Oct. 24). The Parkinson's self-assessment tool
[8] G. Ebersbach, H. Baas, I. Csoti, M. M¨ungersdorf, and G. Deuschl, "Scales
in Parkinson's disease," J. Neurol., vol. 253, no. 4, pp. iv32–iv35, 2006.
[30] B. Peek, (2011, Oct. 24). Managed library for Nintendo's wiimote
[9] Parkinson's UK. (2011, Oct. 24). Tremor and Parkinson's. [Online]. Avail-
[31] Brite Computers. (2011, Oct. 24). Brite classmates [Online]. Available:
[10] J. Synnott, L. Chen, C. D. Nugent, and G. Moore, "WiiPD—An approach
for the objective home assessment of Parkinson's disease," in Proc. 33rdAnnu. Int. Conf. IEEE Eng. Med. Biol. Soc., Aug./Sep. 2011, pp. 2388–2391.
[11] S. Patel, K. Lorincz, R. Hughes, N. Huggins, J. Growdon, D. Standaert,
M. Akay, J. Dy, M. Welsh, and P. Bonato, "Monitoring motor fluctuations
Jonathan Synnott received the B.Sc. degree (Hons.) in computing science from
in patients with Parkinson's disease using wearable sensors," IEEE Trans.
the University of Ulster, Jordanstown, U.K., in 2009. He is currently working
Inf. Technol. Biomed., vol. 13, no. 6, pp. 864–873, Nov. 2009.
toward the Ph.D. degree at the University of Ulster in the assessment and
[12] J. P. Giuffrida, D. E. Riley, B. N. Maddux, and D. A. Heldman, "Clini-
visualization of sensor data for monitoring within intelligent environments.
cally deployable KinesiaTM technology for automated tremor assessment,"
His research interests include data visualization and motor analysis.
Movement Disorders, vol. 24, pp. 723–730, 2009.
[13] A. Salarian, H. Russmann, F. J. G. Vingerhoets, P. R. Burkhard, Y. Blanc,
C. Dehollain, and K. Aminian, "An ambulatory system to quantifybradykinesia and tremor in Parkinson's disease," in Proc. 4th IEEE Int.
Conf. Inf. Technol. Appl. Biomed., 2003, pp. 24–26.
Liming Chen received the B.Sc. and M.Sc. degrees in computing engineering
[14] L. Atallah, B. Lo, R. King, and G. Z. Yang, "Sensor placement for activity
from the Beijing Institute of Technology, Beijing, China, and the D.Phil. degree
detection using wearable accelerometers," in Proc. Int. Conf. Body Sensor
in artificial intelligence from De Montfort University, Leicester, U.K.
Networks, Jun. 2010, pp. 24–29.
He is a Lecturer at the School of Computing and Mathematics, University
[15] K. Niazmand, K. Tonn, A. Kalaras, S. Kammermeier, K. Boetzel,
of Ulster, Jordanstown, U.K. His current research interests include the semantic
J. Mehrkens, and T. Lueth, "A measurement device for motion analy-
technologies, intelligent systems, information/knowledge fusion and reasoning,
sis of patients with Parkinson's disease using sensor based smart clothes,"
context-aware computing, assistive technologies, and their applications in intel-
in Proc. 5th Int. Conf. Pervasive Comput. Technol. for Healthcare (Perva-
siveHealth), May 2011, pp. 9–16.
[16] J. Synnott, L. Chen, C. D. Nugent, and G. Moore, "Assessment and vi-
sualization of Parkinson's disease tremor," in Proc. 10th IEEE Int. Conf.
Inf. Technol. Appl. Biomed., pp. 1–4.
[17] T. Starner, J. Auxier, D. Ashbrook, and M. Gandy, "The gesture pendant:
A self-illuminating, wearable, infrared computer vision system for home
Chris D. Nugent (S'96–A'99–M'03) was born in 1973. He received the B.Eng.
automation control and medical monitoring," in Proc. Int. Symp. Wearable
degree in electronic systems and the D.Phil. degree in biomedical engineering
Comput., 2000, pp. 87–94.
from the University of Ulster, Jordanstown, U.K., in 1995 and 1998, respectively.
[18] C. G. Goetz, G. T. Stebbins, D. Wolff, W. DeLeeuw, H. Bronte-Stewart,
He is Professor of biomedical engineering at the University and his research
R. Elble, M. Hallett, J. Nutt, L. Ramig, T. Sanger, A. D. Wu, P. H. Kraus,
interests include the design and evaluation of smart environments for ambient
L. M. Blasucci, E. A. Shamim, K. D. Sethi, J. Spielman, K. Kubota,
assisted living applications.
A. S. Grove, E. Dishman, and C. B. Taylor, "Testing objective measuresof motor impairment in early Parkinson's disease: Feasibility study of anat-home testing device," Movement Disorders, vol. 24, pp. 551–556, 2009.
[19] J. Westin, M. Dougherty, D. Nyholm, and T. Groth, "A home environment
test battery for status assessment in patients with advanced Parkinson's
George Moore received the B.Sc. degree (Hons.) in computing science and
disease," Comput. Methods Programs Biomed., vol. 98, pp. 27–35, 2010.
the Ph.D. degree in computing science both from the University of Ulster,
[20] S. Keates and S. Trewin, "Effect of age and Parkinson's disease on cursor
Jordanstown, U.K, in 1994 and 2000, respectively.
positioning using a mouse," in Proc. 7th Int. ACM SIGACCESS Conf.
He is a Lecturer at the School of Computing and Mathematics, University of
Comput. Accessibility, 2005, pp. 68–75.
Source: http://www.tech.dmu.ac.uk/~limingchen/TITB%20WiiPD.pdf
The Role of Flavonoids in Osteoarthritis Introduction Humans have used botanical products for medicinal purposes for thousands of years with many of the pharmaceuticals used today derived, in part, from natural substances. Ethnopharmacology has become a major thrust in research and development of new pharmaceutical compounds. Many natural compounds have biologic activity in multiple diseases and physiologic processes from maintaining cardiovascular, renal and gastrointestinal function to safely helping to manage cancer, ulcers, arthritis, and liver disease. Among these safe and effective botanical compounds are flavonoids with more than 9,000 distinct molecular species.
IEEE TRANSACTIONS ON INFORMATION TECHNOLOGY IN BIOMEDICINE, VOL. 16, NO. 6, NOVEMBER 2012 WiiPD—Objective Home Assessment of Parkinson's Disease Using the Nintendo Wii Remote Jonathan Synnott, Student Member, IEEE, Liming Chen, Member, IEEE, Chris. D. Nugent, Member, IEEE, and George Moore, Member, IEEE Abstract—Current clinical methods for the assessment of



