Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Extended release potassium salts overdose and endoscopic removal of a pharmacobezoar: a case report

Contents lists available at
Toxicology Reports
Extended release potassium salts overdose and endoscopic
removal of a pharmacobezoar: A case report
nón Jorge Guillermo , Pérez Hernández Juan Carlos ,
Bautista Albiter Mayré Ivonne , Terán Flores Herminio ,
Ramírez Pérez Rubén
a Jefe del Centro Toxicológico Hospital Angeles Lomas, Vialidad de la Barranca No. 14, Colonia Valle de las Palmas, Huixquilucan, Estado
de México CP 52787, Mexico
b Adscrito al Centro Toxicológico Hospital Angeles Lomas, Vialidad de la Barranca No. 14, Colonia Valle de las Palmas, Huixquilucan,
Estado de México CP 52787, Mexico
c Residente de Toxicología Hospital Angeles Lomas, Vialidad de la Barranca No. 14, Colonia Valle de las Palmas, Huixquilucan, Estado de
México CP 52787, Mexico
Background: Reported cases of potassium overdoses have shown that this condition could
Received 7 February 2014
generate several morbidities, mainly related to cardiac dysrhythmias even with fatal out-
Received in revised form 4 April 2014
comes in some cases.
Accepted 4 April 2014
Potassium salts in extended release tablets could form pharmacobezoars if a large amount
Available online 22 May 2014
is ingested. In relation to the above, when the patient has a pharmacobezoar, clinical find-
ings may be delayed and may persist.
The techniques available for removal of a pharmacobezoar are whole bowel irrigation
(WBI), endoscopy or in some surgery as a decontamination method has
shown promising results.
Extended release potassium salts
Case report: A 42 year old woman, who intentionally ingested 100 tablets of extended release
potassium chloride, 50 mg of clonazepam and an undisclosed amount of ethanol, presented
with metabolic acidosis, hyperlactatemia and sinus tachycardia 2 h after ingestion. Gastric
lavage and activated charcoal were applied initially, specific measures were not neces-
sary. However, a transcutaneous pacemaker was placed. Because of her background, we
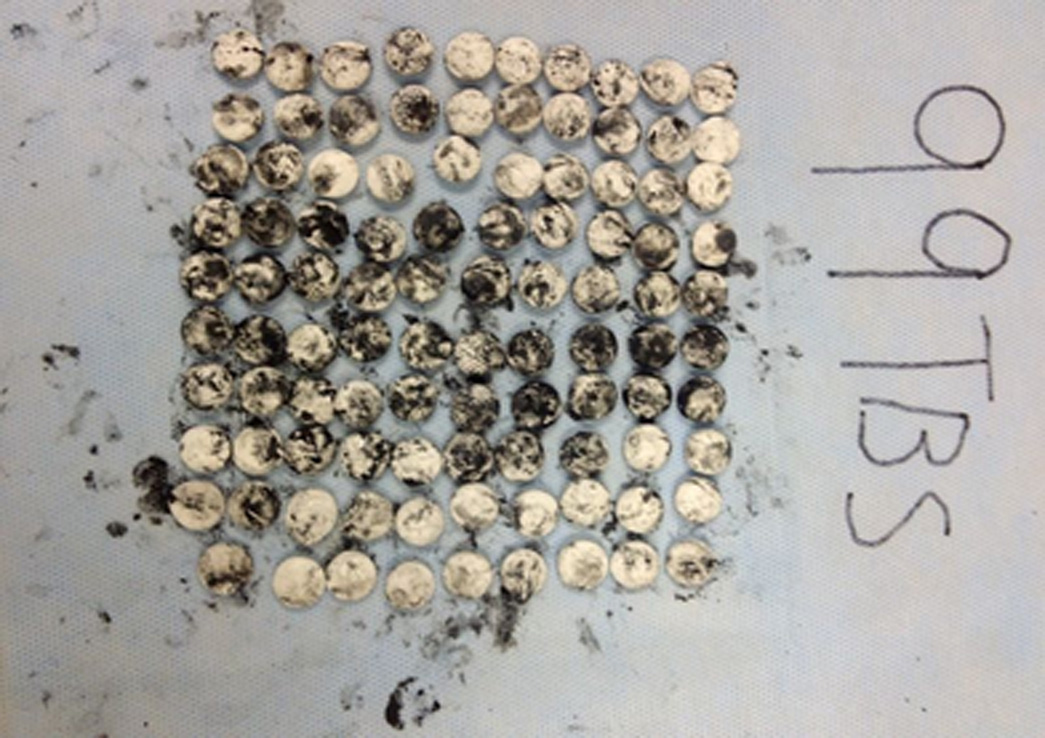
considered a pharmacobezoar and an endoscopy were performed to remove 99 tablets of
potassium that were isolated or forming concretions.
Discussion: The readily available techniques to remove a pharmacobezoar are whole bowel
irrigation (WBI) and endoscopy; nevertheless there is not a consensus about their relative
merits. Our patient was treated by endoscopy because we found on the X-ray a conglom-
erate of radiopaque images suggesting a pharmacobezoar. In this case we did not have any
adverse effect.
Conclusions: We consider that endoscopy could be an effective and safe method to remove
a drug bezoar from the stomach in uncomplicated patients.
2014 he Authors. Published by Elsevier Ireland Ltd. This is an open access article under
the CC BY-NC-ND license (
∗ Corresponding author. Tel.: +52 1 55 52465056; mobile: +52 1 55 19177028.
E-mail addresses: (P.T.J. Guillermo), (P.H.J. Carlos),
(B.A.M. Ivonne), (T.F. Herminio), (R.P. Rubén).
Mobile: +52 1 55 48706380.
Mobile: +52 1 722 5189242.
Mobile: +52 1 55 39896337.
Mobile: +52 1 55 45832697.
2214-7500/ 2014 he Authors. Published by Elsevier Ireland Ltd. This is an open access article under the CC BY-NC-ND license (

P.T.J. Guillermo et al. / Toxicology Reports 1 (2014) 209–213
Extended release potassium salts are indicated in
induced or acquired hypokalemic conditions. The potas-
sium overdose could generate hyperkalemic states, espe-
cially if the patient has impaired renal function or if there
has been a large ingestion of salts (toxic dosage: 2 mEq/kg)
a patient presents a large ingestion of extended
release potassium tablets, clinical manifestations could be
delayed even more than 24 h and concretions could be
formed in the stomach. Concretions complicates the decon-
tamination by gastric lavage, so that after this procedure in
these patients, it is possible to find tablets remaining in the
stomach, even in 88.2% of cases
The great absorption that follows to a massive ingestion
of potassium salts causes myocardial conduction distur-
bances and metabolic acidosis.
The correct technique for gastrointestinal decontami-
nation in cases of massive overdose of extended-release
tablets is not well established, nowadays, toxicologists con-
tinue to consider use of whole bowel irrigation (WBI),
endoscopy or even surgery to evacuate tablet remaining
from the stomach
Fig. 1. Abdominal radiography with multiple radioopacities in the stom-
ach (red arrow).
2. Case report
A 42 year old woman with history of borderline person-
ality disorder and a suicide attempt with potassium salts
(50 tablets) one year earlier presented to the emergency
room after intake of 100 tablets of extended release potas-
sium chloride (1000 mEq), 50 mg of liquid clonazepam, and
an undisclosed amount of ethanol at home.
She recognized this as a new suicide attempt and pre-
sented with somnolence, tachycardia and exhalation of
ethanol odor 2 h after ingestion. Her vital signs were: blood
pressure 130/90 mm Hg, pulse was 97 beats/min, respira-
tions were 22 breaths/min, temperature was 36.5 ◦C, and
oxygen saturation was 98% on room air.
A 12 lead electrocardiogram demonstrated sinus tachy-
cardia with normal QRS duration and unaltered T-waves.
Potassium level was 3.9 mmol/L, blood gas analysis
revealed pH 7.25, HCO3 17.5 mEq/L and lactate 4.9 mmol/L.
A standard toxicological screen was negative for all agents.
Ethanol level was 90.80 mg/dl. Finally a plain film of the
abdomen showed multiple opacities in the region of the
stomach (Other agents, including acetaminophen
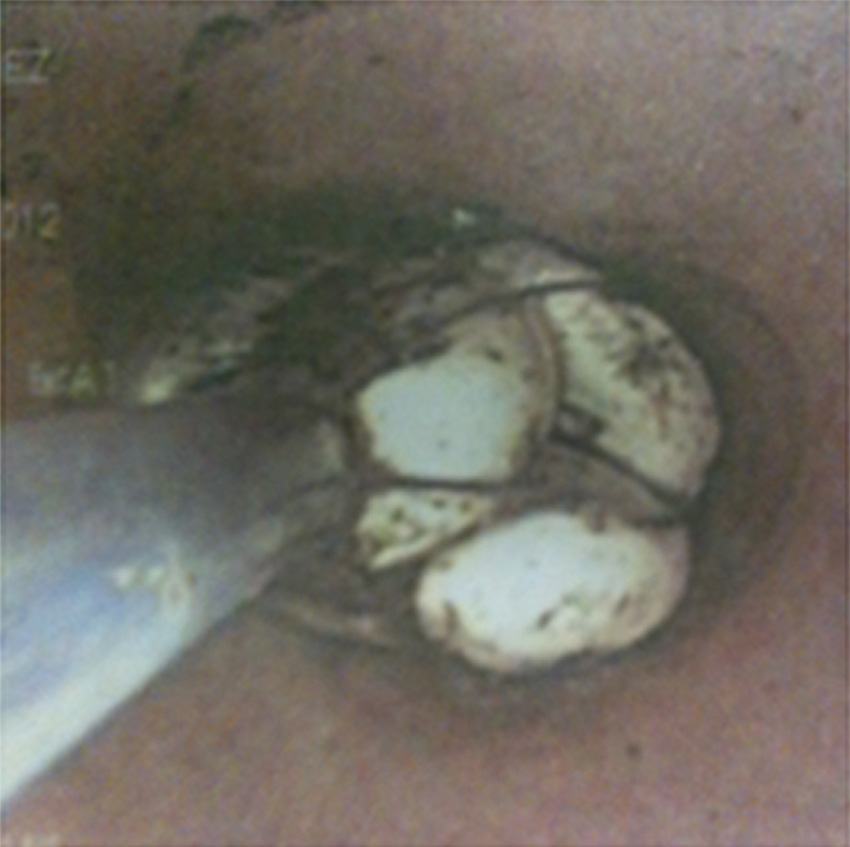
Fig. 2. Endoscopic removal of the tablets.
and salicylates were reported to be absent.
A venous access was placed. After that, a gastric lavage
A total of 99 of the 100 tablets that were either isolated
with a 20-french orogastric tube (maximum size in our hos-
or forming concretions were removed with an endoscopic
pital) was performed. However, no tablets were recovered
during this procedure. Also, a single dose of activated char-
After gastric decontamination, clinical outcome was sat-
coal was performed in order to treat a possible coingestant.
isfactory, pharmacological correction of acidosis was not
Anti-hyperkalemic measures were not necessary at that
needed and she did not develop hyperkalemia or cardio-
time. However, a transcutaneous pacemaker was placed.
vascular impairments. The patient was intubated for the
Given her background and the gastric lavage that was
procedure and extubated 18 h later. After that, she was
ineffective, an abdominal radiography was performed in
discharged to the psychiatry service 48 h later.
order to identify the location of the tablets. The radiography
showed multiple radiopacities in the stomach and the pos-
sibility of a pharmacobezoar was considered. Consultation
with the gastroenterology service was done to request an
The potassium excess could be absorbed by the intra-
endoscopy for removal of the suspected pharmacobezoar.
cellular compartment to maintain serum levels under
P.T.J. Guillermo et al. / Toxicology Reports 1 (2014) 209–213
Fig. 3. Removed tablets.
5.5 mEq/L, but unfortunately this mechanism is saturable
We considered the high risk of massive absorption with
this context, potassium serum levels over 6.0 mEq/L
hemodynamic implications and started management with
should be considered risky and need to be treated immedi-
airway protection, placement of a pacemaker and decon-
ately there is no clear relationship between
tamination by endoscopy Furthermore, our patient
the serum level and heart rhythm disturbances, we know
had a history of a previous suicide attempt with 50 tablets
that the risk of dysrhythmias is increased if rapid absorp-
of extended release potassium salts. She developed hyper-
tion of potassium occurs
kalemia, metabolic acidosis and hyperacute T waves, and
Many drugs are capable to form concretions as in
was hospitalized seven days in an intensive care unit. In
the case of amitriptyline, salicylates, carbamazepine, iron,
the second attempt, even though the patient increased
potassium salts and other extended release preparations,
the ingestion to 100 tablets of the same drug, she did not
with or without an enteric coat
develop any complication and was discharged two days
The gastric decontamination is an essential procedure
after ingestion. We strongly concur that if a pharmacobe-
in the treatment of patients with an oral drug overdose;
zoar is suspected endoscopy should be considered in order
however, the appropriate technique to remove a bezoar is
to avoid a massive absorption
On the other hand, the multiple introductions of the
The gastric lavage and activated charcoal administra-
endoscope could increase the risk of airway injuries and
tion have both been demonstrated to be poorly effective on
aspiration of gastric content that, in our case,
patients with pharmacobezoars. Moreover, in Mexico there
the equipment was introduced eighteen times and no com-
are no orogastric tubes with a recommended diameter to
plications were presented. For this reason, we consider the
remove extended release tablets (36–40 Fr).
endoscopic removal of bezoars a therapeutical option for
Nowadays, the available techniques to remove phar-
macobezoars include: WBI (only small size bezoars),
endoscopy and surgical extraction. In this context, the
Case development.
main factors to consider before selecting a decontamina-
tion technique are: drug toxicity, pharmacobezoar size and
location, clinical condition of the patient and availability of
the resources (polyethylene glycol, operating room, etc.)
Parenteral solutions
Not Anti hyperkalemic
Despite the fact that WBI has been demonstrated in
some reports be safe and to improve the clinical condition
of these patients, at this time there is no strong evidence of
its efficacy. It requires several hours to clarify the effluent,
(after endoscopy)
also, it is necessary to have a normal bowel function and
it could not be effective if a big bezoar exists in the stom-
ach. In the case of perforation, intestinal occlusion, active
bleeding, hemodynamic instability or vomiting, the WBI
are contraindicated in the case of a potassium
salts overdose, one of the most important causes of morbid-
Not Anti hyperkalemic
ity is the cardiac rhythm disturbance with hemodynamic
measures. Transcutaneous
instability, which limits the use of WBI.
pacemaker was removed
P.T.J. Guillermo et al. / Toxicology Reports 1 (2014) 209–213
uncomplicated patients and should be performed early if
the medical center is short of appropriate orogastric tubes
This was a case of intentional potassium, ethanol and
Gunja a case of a patient who ingested
clonazepam overdose resulting in mild metabolic acidosis,
100 tablets of extended release potassium chloride with
hyperlactatemia and sinus tachycardia at 2 h after inges-
severe hyperkalemia 5 h after the ingestion Also,
tion, without hyperkalemia and after utilizing endoscopy
Saxena a case of a woman who ingested
in order to remove 100 isolated tablets and forming phar-
16 mEq/Kg of potassium salts and developed severe hyper-
macobezoars. In this case, the bezoar formation could lead
kalemia with cardiac arrest in the first hour after the
to massive absorption of potassium and increase the risk of
ingestion. Finally, Colledge another case with
hyperkalemic disturbances. In addition to standard treat-
an intake of approximately 100 tablets with hyperkalemia
ments for hyperkalemia, this case report demonstrates
and ventricular tachycardia demonstrating the effects of a
the benefit from endoscopy in extended-release potassium
rapid absorption in massive ingestions of potassium salts.
bezoar formation, considering the hospital resources, time
In our case, due to the early endoscopic removal of tablets,
from the ingestion and clinical status of the patient. Also,
the patient did not increase potassium serum levels and
this study asks whether endoscopy should be used as an
complications were not registered.
initial measure of decontamination in patients who have
Reported cases.
Extended release KCl
Charles et al. (1978)
Illingworth (1980)
Wide complex tachycardia
Colledge et al. (1988)
Hyperacute T waves, sinus
tachycardia 110×.
Ventricular tachycardia
1st degree AV blockade,
hyperacute T waves
Peeters et al. (1998)
300 tabs (2.4 mmol)
Abdominal distension. One
month later gastric
20 tabs of extended
Left ventricular heart
release KCl (630 mg).
Bendoflurazide and
Unaltered EKG. Nausea and
vomiting, Asystole, death
in gastric lavage
40 tabs of extended
release KCl (8 mmol)
Whitaker et al. (2000)
Tachycardia (155×) 1st
degree AV blockade.
Hyperacute T waves
100 tabs (10 mEq)
Hyperacute T waves
20–30 tabs (10 mEq)
Tachycardia, nausea,
vomiting and diarrhea
Asthenia and adinamia
Tachycardia (100×)
Tachycardia (124×)
10–20 tab (8 mmol)
4, 5, 6, 7, 8.
1, 5, 6, 7, 9, 11, 14.
Briggs Albert et al. (2013)
Mildly peaked T waves
2, 3, 5, 6, 7, 8.
Pérez et al. (2013)
Metabolic acidosis,
hyperlactatemia and sinus
tachycardia with normal T
1: gastric lavage; 2: whole bowel irrigation; 3: endoscopy; 4: hemodialysis; 5: calcium; 6: insulin/glucose; 7: sodium bicarbonate; 8: -2 agonist; 9: ion
exchange resin; 10: furosemide; 11: activated charcoal; 12: mannitol; 13: cardiac pacemaker and 14: advanced cardiac resuscitation.
P.T.J. Guillermo et al. / Toxicology Reports 1 (2014) 209–213
ingested a large quantity of tablets, particularly in centers
where there is a lack of adequate tubes for gastric lavage
We concur that in selected cases endoscopy could be
used instead of gastric lavage as first decontamination mea-
sure, although, a clinical guideline for the use of endoscopy
as a decontamination method still need to be created.
Cases of extended release potassium salts reported are
summarized below (
Conflict of interest
The authors declare that they have no competing inter-
Special thanks to Dr. Carlos Mitrani Boyle, gastroen-
terologist and endoscopist who performed the procedure.
Appendix A. Supplementary data
Supplementary data associated with this article can
be found, in the online version, at
Source: http://www.retomex.org.mx/wp-content/uploads/2014/05/toxicology-reports.pdf
GASTROENTEROLOGY 2011;140:116 –123 Histomorphometric Analysis Reveals Reduced Bone Mass and BoneFormation in Patients With Quiescent Crohn's Disease ANGELA E. OOSTLANDER,* NATHALIE BRAVENBOER,*,‡ EVELIEN SOHL,* PAULIEN J. HOLZMANN,*CHRISTIEN J. VAN DER WOUDE,§ GERARD DIJKSTRA,储 PIETER C. F. STOKKERS,¶ BAS OLDENBURG,#J. COEN NETELENBOS,* DANIEL W. HOMMES,** AD A. VAN BODEGRAVEN,‡‡ and PAUL LIPS* on behalf of the
© SUPPLEMENT TO JAPI • FEBRUARY 2013 • VOL. 61 Management of Hypertension Goals of Therapy • In low risk patients, it is suggested to institute life style modifications and observe BP for a period of 2-3 months, he primary goal of therapy of hypertension should be before deciding whether to initiate drug therapy. effective control of BP in order to prevent, reverse or delay



