Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Icc-ibd.stijlloos.nl
GASTROENTEROLOGY 2011;140:116 –123
Histomorphometric Analysis Reveals Reduced Bone Mass and Bone
Formation in Patients With Quiescent Crohn's Disease
ANGELA E. OOSTLANDER,* NATHALIE BRAVENBOER,*,‡ EVELIEN SOHL,* PAULIEN J. HOLZMANN,*CHRISTIEN J. VAN DER WOUDE,§ GERARD DIJKSTRA,储 PIETER C. F. STOKKERS,¶ BAS OLDENBURG,#J. COEN NETELENBOS,* DANIEL W. HOMMES,** AD A. VAN BODEGRAVEN,‡‡ and PAUL LIPS* on behalf of the
Dutch Initiative on Crohn and Colitis (ICC)
*Department of Endocrinology, VU University Medical Center, Research Institute MOVE, Amsterdam; Departments of ‡Clinical Chemistry and ‡‡Gastroenterology andHepatology, VU University Medical Center, Amsterdam; §Department of Gastroenterology and Hepatology, Erasmus Medical Center, Rotterdam; 储
Department ofGastroenterology and Hepatology, University Medical Center Groningen, University of Groningen, Groningen; ¶Department of Gastroenterology and Hepatology,Academic Medical Center, Amsterdam; #Department of Gastroenterology and Hepatology, University Medical Center Utrecht, Utrecht; and **Department ofGastroenterology and Hepatology, Leiden University Medical Center, Leiden, The Netherlands
See related article, on page
Patients with inflammatory bowel disease (IBD), in
particular patients with Crohn's disease (CD), are at
30 in CGH; see editorial on page 22.
increased risk for bone loss. The prevalence of osteopeniaand osteoporosis in patients with IBD varies betweenstudies and is reported to be up to 42% and 16%, respec-
BACKGROUND & AIMS: Crohn's disease (CD) is asso-
The pathogenesis of bone loss in patients with
ciated with an increased prevalence of osteoporosis, but the
IBD is complex, multifactorial, and only partly under-
pathogenesis of this bone loss is only partly understood. We
stood. General risk factors such as malnutrition, malab-
assessed bone structure and remodeling at the tissue level in
sorption, calcium and vitamin D deficiency, and cortico-
patients with quiescent CD. We also investigated the roles
steroid treatment are known to be However,
of osteocyte density and apoptosis in CD-associated bone
these factors cannot completely explain the bone loss.
loss.
METHODS: The study included 23 patients with
Recently, the inflammatory process itself has been sug-
quiescent CD; this was a subgroup of patients from a large
gested to play a pivotal role in IBD-associated bone loss.
randomized, double-blind, placebo-controlled, multicenter
For example, proinflammatory cytokines that contribute
trial. We obtained transiliac bone biopsy samples and per-
to the intestinal immune response in IBD, such as tumor
formed histomorphometric analysis. Results were com-
necrosis factor ␣ and factors belonging to the receptor
pared with data from age- and sex-matched healthy individ-
activator for nuclear factor B ligand (RANKL)/osteopro-
uals (controls).
RESULTS: Trabecular bone volume was
tegerin system, are known to enhance bone
decreased among patients with CD compared with controls
Bone remodeling involves a balanced process of bone
(18.90% vs 25.49%;
P ⬍ .001). The low bone volume was
resorption by osteoclasts and subsequent bone formation
characterized by decreased trabecular thickness (120.61 vs
by osteoblasts. An imbalance in this process can be as-
151.42 m;
P ⬍ .01). Bone formation and resorption were
sessed by measurement of biochemical markers of bone
reduced, as indicated by a decreased mineral apposition rate
turnover. In patients with IBD, bone resorption is in-
(0.671 vs 0.746 m/day;
P ⬍ .01) and a low osteoclast
creased, as indicated by elevated levels of the markers
number and surface area compared with controls and pub-
deoxypyridinoline and cross-linked N-telopeptide of type
lished values, respectively. In trabecular bone of patients
1 Bone formation in patients with IBD is less
with CD, osteocyte density and apoptosis were normal. The
well characterized. Increased levels of (bone-specific) al-
percentage of empty lacunae among patients was higher
kaline decreased levels of
than that of published values in controls.
CONCLU-
and normal levels of bone formation markers have been
SIONS: In adult patients with quiescent CD, bone his-
reported in patients with Therefore, based on
tomorphometric analysis revealed a reduction in bone
biochemical markers of bone turnover, the bone remod-
mass that was characterized by trabecular thinning. The
CD-associated bone loss was caused by reduced bone
formation, possibly as a consequence of decreased os-
Abbreviations used in this paper: 25(OH)D, 25-hydroxyvitamin D3;
ALP, alkaline phosphatase; CD, Crohn's disease; CDAI, Crohn's Dis-
teocyte viability in the patients' past.
ease Activity Index; IBD, inflammatory bowel disease; RANKL, receptor
Keywords: Bone Histomorphometry; Osteocyte Apoptosis;
activator for nuclear factor kappa B ligand; TNF, tumor necrosis factor.
2011 by the AGA Institute
Inflammatory Bowel Disease; Osteoporosis.
BONE HISTOMORPHOMETRY IN QUIESCENT CD
eling balance in patients with IBD is characterized by a
patients with CD and is believed to progress to (presenile)
net increase of bone resorption.
osteoporosis. Hence, as such it is the most relevant pop-
At the tissue and cellular level, low bone mass is caused
ulation to study. Of the 23 patients included, 12 were
by a disturbed regulation of bone remodeling as
women, of whom one was postmenopausal. Patients with
Histomorphometric analysis of bone biopsy specimens is
current or recent bisphosphonate or corticosteroid treat-
a powerful tool to show disturbances in bone remodel-
ment (⬍1 year and ⬍3 months, respectively, before in-
ing. In patients with IBD, there are only few data con-
clusion) were excluded, as well as patients with known
cerning bone histomorphometry. Croucher et al showed
metabolic bone diseases and serum levels of 25-hy-
reduced bone formation and a mild mineralization defect
droxyvitamin D3 less than 25 nmol/L. The study was
in patients with IBD who had Ward et al
approved by the institutional review board at each par-
observed both a suppressed bone formation and bone
ticipating medical center. All patients gave written in-
resorption in children with newly diagnosed
formed consent.
whereas Hessov et al reported normal bone remodelingand mineralization in young patients with
The regulation of bone remodeling is believed to be
Biochemical measurements in serum included cal-
supervised by osteocytes, the third cell type in bone in
cium (colorimetric assay; Roche Diagnostics, Mannheim,
addition to osteoblasts and osteoclasts. As a conse-
Germany), 25-hydroxyvitamin D3 (radioimmunoassay;
quence, a lack of functionally active osteocytes might
DiaSorin, Stillwater, MN), C-reactive protein (immuno-
underlie bone pathology. In fact, the number of osteo-
turbidimetric assay; Roche Diagnostics), and total alka-
cytes appears to decline with and is lower in
line phosphatase (International Federation of Clinical
postmenopausal women, especially in those with a
Chemistry method; Roche Diagnostics). Intra-assay and
vertebral fracture, when compared with premenopausal
inter-assay coefficients of variation of the assays were as
Moreover, the percentage of apoptotic osteo-
follows: calcium, 0.9% and 1.3%; 25-hydroxyvitamin D3,
cytes in postmenopausal women has been shown to be
8% and 10%; C-reactive protein, 1.2% and 1.4%; and alka-
associated with the level of bone Informa-
line phosphatase, 0.7% and 2.4%. Measurements were
tion on osteocyte density and osteocyte function in bone
performed by the laboratories of Clinical Chemistry and
of patients with IBD is lacking thus far.
Endocrinology of the VU University Medical Center.
To ascertain a better understanding of bone biology in
patients with IBD, the aims of this study were to (1)
assess bone structure and remodeling at the tissue level in
Patients received 2 doses of tetracycline (250 mg
patients with quiescent CD in comparison with healthy
4 times daily) for 2 days separated by an interval of 10
controls and (2) investigate whether osteocyte density
days. Three to 7 days after the last dose, transiliac bone
and osteocyte apoptosis are related to bone structure and
biopsy specimens were taken using Bordier's trephine
(ID, 8 mm). The bone biopsy specimens were fixed in cold4% phosphate-buffered formaldehyde, dehydrated in gradedethanol, and embedded in 80% methylmethacrylate (BDH
Patients and Methods
Chemicals, Poole, England) supplemented with 20% dibuth-
ylphtalate (Merck, Darmstadt, Germany), 8 g/L lucidol CH-
Twenty-three patients with quiescent CD partici-
50L (Akzo Nobel, Deventer, The Netherlands), and 22
pated in this study. These patients were a subgroup
L/10 mL
N,N dimethyl-p-toluidine (Merck). Five-micro-
included in a large randomized, double-blind, placebo-
meter-thick undecalcified sections were cut with a Polycut
controlled, multicenter trial on the effect of risedronate
2500 S microtome (Reichert–Jung, Nussloch, Germany).
in patients with quiescent CD who had osteopenia (N ⫽
Goldner's trichrome stain was performed to distinguish
131, Crohn and Bone Study). The current study describes
between calcified bone and noncalcified matrix (osteoid).
data obtained from patients at baseline. Patients were
Tartrate-resistant acid phosphatase stain was used to visu-
diagnosed with CD using clinical, endoscopic, histologic,
alize osteoclasts. Unstained sections were used for fluores-
and radiologic criteria according to Pa-
cence microscopy to measure tetracycline labels.
tients had to be in remission (Crohn's Disease ActivityIndex [CDAI] ⬍150). Although 2 patients had a CDAI
⬎150, these patients had absence of symptoms of active
Apoptotic cells were visualized by immunohisto-
disease and no signs of active inflammation on sigmoid-
chemical detection of activated caspase-3. Immunohisto-
oscopy and as such were defined to be in clinical remis-
chemistry was performed on two 5-m sections of each
sion. Another inclusion criterion was a lumbar spine
biopsy specimen, which were obtained with an interval of
and/or total hip bone mineral density with a T-score of
30 m. Sections were cut and transferred to poly-L-
⫺1 to ⫺2.5 SD (osteopenia). Osteopenia is the most
lysine– coated slides. After deplastification and rehydra-
prevalent state of bone loss in usually relatively young
tion, sections were decalcified for 10 minutes with 1%
GASTROENTEROLOGY Vol. 140, No. 1
acetic acid. Antigen retrieval was performed by a
lacunae per bone area, total number of lacunae per bone
30-minute incubation with 0.5% saponin (Sigma, St
area, percentage of positive osteocytes per total number
Louis, MO) in phosphate-buffered saline (PBS) and a
of osteocytes, and percentage of empty lacunae per total
10-minute incubation with 3.5 g/mL deoxyribonuclease
number of lacunae.
II (Sigma) in 25 mmol/L Tris plus 10 mmol/L magne-
To compare the data of this CD population with
sium sulfate. Sections were incubated with 3% hydrogen
healthy controls, we used healthy control data from 17
peroxide in methanol to block endogenous peroxidase
men and 26 women (aged 20 – 60 kindly provided
and with 5% normal goat serum in PBS plus 0.05%
by Prof Dr J. E. Compston (Cambridge, England). From this
Tween20 to block nonspecific binding sites. Incubation
population, sections of 10 age- and sex-matched healthy
with primary antibody was performed overnight at 4°C
controls were measured to verify comparability of the his-
with 1/75 rabbit anti-cleaved caspase-3 antibody (Cell
tomorphometric indices. The systemic measurement differ-
Signaling Technology, Beverly, MA) in PBS plus 0.05%
ence between our measurements and those from England
Tween20. Sections were then incubated for 1 hour with
was as follows: bone volume, 0.93; trabecular thickness,
1/100 biotin-labeled goat anti-rabbit immunoglobulin G
0.88; trabecular number, 0.99; osteoid volume, 0.93; and
(Vector Laboratories, Burlingame, CA) in PBS plus 0.05%
osteoid thickness, 0.98.
Tween20. Subsequently, the sections were incubated for30 minutes with the ABC kit (Vector Laboratories) and
developed for 10 minutes with 3,3=-diaminobenzidine
Results are expressed as mean ⫾ SD. Histomor-
with nickel enhancement. Finally, sections were counter-
phometric indices were compared between patients with
stained with 0.025% toluidine blue in water, dehydrated,
CD and healthy controls, as well as between men and
and sealed in DePeX mounting medium (BDH Chemi-
women using a 2-tailed Student
t test for independent
cals, VWR International, Poole, England).
samples. Correlations between histomorphometric pa-rameters and biochemical indices were calculated using
Pearson's coefficient of correlation. All statistical analyses
Histomorphometry was performed mainly on tra-
were performed using SPSS software (version 15.0; SPSS
becular bone. Static histomorphometry was performed
Inc, Chicago, IL). A
P value of ⬍.05 was considered
automatically using NIS-Elements AR 2.10 (Nikon
¨sseldorf, Germany) at 100⫻ magnification.
Dynamic histomorphometry was performed semiauto-
matically using OsteoMeasure (Osteometrics, Atlanta,
GA). All measurements were performed according to theAmerican Society of Bone and Mineral Research nomen-
Patient characteristics are listed in Be-
Mean cortical thickness was assessed manually
cause several parameters showed relatively high variation
by measuring both cortices, each at 4 equidistant places.
in the total population, data are presented for men and
Trabecular bone volume, trabecular bone surface, and
women separately. The quiescent state of disease in our
trabecular thickness were measured and used to calculate
CD population was ascertained by a mean CDAI of
trabecular number and trabecular separation. Besides
93.8 ⫾ 71.7 and a mean C-reactive protein level of 7.3 ⫾
these structural indices, parameters associated with bone
8.4 mg/L. Disease activity was similar in men and women
formation were measured, including osteoid volume, os-
with CD. Disease duration tended to be longer in male
teoid surface, and osteoid thickness. Furthermore, the
patients with CD (
P ⫽ .067). Levels of biochemical pa-
distance between double tetracycline labels and the la-
rameters were all within the reference values of our lab-
beled (mineralizing) surface was measured under UV
oratory. However, alkaline phosphatase levels in men
light and used to calculate mineral apposition rate, bone
with CD were at the upper limit of the reference range
formation rate, adjusted apposition rate, and mineraliza-
and were higher than alkaline phosphatase levels in
tion lag time. Bone resorption was assessed as osteoclast
women with CD (86 vs 60 IU/L;
P ⫽ .003).
number (measured manually using an integrated eye-piece, Zeiss II; Zeiss, Oberkochen, Germany) and osteo-
clast surface. All measurements were performed by one
Histomorphometric data concerning bone struc-
ture are summarized in Trabecular bone volume
In addition, the total number of osteocytes, the num-
and trabecular thickness were reduced in patients with
ber of cleaved caspase-3–positive osteocytes, and the
CD when compared with healthy controls (
P ⬍ .001 and
number of empty lacunae in the entire trabecular bone
P ⫽ .006, respectively; and
B). Trabecular
area were counted at 200⫻ magnification. Duplicate sec-
number was unaffected. Comparison of bone structure
tions were analyzed by the same investigator. From these
parameters between men and women showed no differ-
data, the following parameters were calculated: total
ences within the control population. However, in patients
number of osteocytes per bone area, number of empty
with CD, trabecular bone volume tended to be lower in
BONE HISTOMORPHOMETRY IN QUIESCENT CD
Table 1. Patient Characteristics
Body mass index (
kg/m2)
82 ⫾ 61 (0–194)
105 ⫾ 81 (6–322)
C-reactive protein level (
mg/L)
a
6.6 ⫾ 6.2 (1–17)
7.9 ⫾ 10.3 (1–38)
Location of disease
Large intestine/small intestine/both
Bowel resection, yes/no (n)
Disease duration (
y)
Age at diagnosis (
y)
Mesalamine derivatives
25-Hydroxyvitamin D3 (
nmol/L)
a
Alkaline phosphatase (
U/L)
a
86 ⫾ 25
b,
c
Bone mineral density lumbar spine (
g/cm2)
Bone mineral density total hip (
g/cm2)
NOTE. Data represent mean ⫾ SD; in the case of CDAI and C-reactive protein, ranges are shown in parentheses.
aReference ranges obtained from the Department of Clinical Chemistry of the VU University Medical Center: C-reactive protein, ⬍8 mg/L;25-hydroxyvitamin D3, 25–150 nmol/L; calcium, 2.20 –2.60 mmol/L; alkaline phosphatase, ⬍120 IU/L.
bN ⫽ 10; alkaline phosphatase value of one patient with a liver function test abnormality was excluded.
cSignificantly different from women with CD (
P ⬍ .01).
men compared with women (
P ⫽ .056). Trabecular num-
in patients with CD when compared with healthy con-
ber was lower in men than in women with CD (
P ⫽ .037),
trols (
P ⫽ .007; ). None of the patients had
and trabecular separation was higher in men (
P ⫽ .049).
signs of osteomalacia. Osteoid volume, mineralizing sur-
In data of male and female patients with CD are
face, and bone formation rate were comparable between
summarized, including variables that were only available
healthy controls and patients with CD ,
D, and
in patients with CD.
F). However, analysis of the individual data revealed a
Histomorphometric data concerning bone remodeling
cluster of 9 patients with CD who had a very low min-
are shown in Mineral apposition rate was lower
eralizing surface (3.78 ⫾ 1.80) as well as bone formation
Table 2. Bone Structure and Remodeling Parameters in Healthy Controls and Patients With CD
Abbreviation (unit)
Controls (n ⫽ 43)
Patients with CD (n ⫽ 23)
18.90 ⫾ 5.28
a
Trabecular thickness
Tb.Th (
m)
120.61 ⫾ 22.16
b
Trabecular number
Tb.N (/
mm)
Osteoid thickness
O.Th (
m)
Mineralizing surface
Mineral apposition rate
MAR (
m/day)
0.671 ⫾ 0.098
b
Bone formation rate
Adjusted apposition rate
Aj.Ar (
m/day)
Mineralization lag time
NOTE. Data represent mean ⫾ SD.
aSignificantly different from the control group (
P ⬍ .001).
bSignificantly different from the control group (
P ⬍ .01).

GASTROENTEROLOGY Vol. 140, No. 1
Figure 1. Histomorphometric measurements on bone structure and remodeling in healthy controls and patients with CD. (A) Bone volume (BV/TV)
is decreased in patients with CD. (B) Trabecular thickness is decreased in patients with CD. (C) Osteoid volume (OV/BV) is unaffected in
patients with CD. (D) Mineralizing surface (MS/BS) is unaffected in patients with CD; however, a subset of 9 patients with CD had a very low
mineralizing surface. (E) Mineral apposition rate (MAR) is decreased in patients with CD. (F) Bone formation rate (BFR) is unaffected in patients with
CD; however, a subset of 9 patients with CD had a very low bone formation rate.
rate (0.022 ⫾ 0.011) in comparison with both the total
patients had a low osteoid volume (0.42 ⫾ 0.34), a low
CD population and healthy controls. Moreover, the 9
number of osteoclasts and osteoclast surface (0.19 ⫾ 0.22
patients in this subgroup (4 men and 5 women; age, 43 ⫾
and 1.36 ⫾ 0.80, respectively), a low mineral apposition
13 years) turned out to have a low bone volume (15.47 ⫾
rate (0.59 ⫾ 0.08), and a low adjusted apposition rate
2.90), which was accompanied by a low total hip bone
(0.29 ⫾ 0.16). Comparison of bone remodeling parame-
mineral density (T-score, ⫺1.38 ⫾ 0.55). Trabecular thick-
ters between men and women showed no statistically
ness and trabecular number were low as well (104.61 ⫾
significant differences in both healthy controls and pa-
16.05 and 1.68 ⫾ 0.33, respectively). Furthermore, these
tients with CD. Examination of the relationship between
Table 3. Bone Structure and Remodeling Parameters in Male and Female Patients With CD
Abbreviation (unit)
Cortical thickness
Ct.Th (m)
16.79 ⫾ 4.58a
Trabecular thickness
Tb.Th (m)
Trabecular number
Tb.N (/mm)
1.63 ⫾ 0.30b
Trabecular separation
Tb.Sp (m)
522.9 ⫾ 116.6b
Osteoid thickness
O.Th (m)
Osteoclast number
N.Oc/TA (/mm2)
Osteoclast surface
Oc.S/BS (%)
Mineralizing surface
Mineral apposition rate
MAR (m/day)
Bone formation rate
Adjusted apposition rate
Aj.Ar (m/day)
Mineralization lag time
NOTE. Data represent mean ⫾ SD.
aTendency towards significantly different from women with CD (P ⫽ .056).
bSignificantly different from women with CD (P ⬍ .05).
BONE HISTOMORPHOMETRY IN QUIESCENT CD
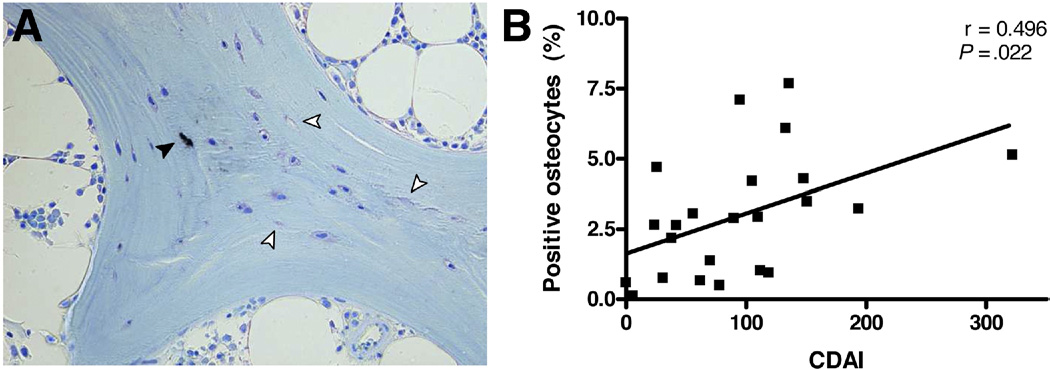
Figure 2. Osteocyte apoptosis in patients with CD. (A) Immunohistochemical staining of a bone biopsy section for cleaved caspase-3. The black
arrowhead indicates an apoptotic osteocyte, and white arrowheads indicate empty lacunae. (B) Positive correlation between disease activity (CDAI)
and the percentage of apoptotic osteocytes.
any of the histomorphometric parameters and disease
controls. Bone remodeling parameters did not differ be-
activity did not reveal statistically significant correlations.
tween sexes.
Also, no correlations were found between other biochem-
The observed low bone mass in patients with quiescent
ical parameters and any of the histomorphometric indi-
CD is in agreement with previous studies on bone histo-
morphometric analysis in patients with Weshowed that the mild bone mass deficit in patients with
quiescent CD is related to thinning of trabeculae. Only
Staining for cleaved caspase-3 clearly visualized
one other study published details on bone microarchi-
apoptotic osteocytes, as depicted in . In this
tecture in patients with IBD, reporting a mild cortical
figure, empty lacunae can be identified as well. In trans-
bone deficit but a normal amount and structure of tra-
iliac bone biopsy specimens of patients with CD, the total
becular bone in children with newly diagnosed In
lacunar density was 293 ⫾ 87 per mm2 bone consisting of
our study, cortical thickness in bone of patients with CD
265 ⫾ 76 osteocytes per mm2 bone and 28 ⫾ 11 empty
was comparable to values in healthy controls (J. Comp-
lacunae per mm2 bone. The percentage of empty lacunae
ston, personal communication). This discrepancy might
over the total number of lacunae was 9.27% ⫾ 3.43%. The
be due to a different response of the developing skeleton
number of positive osteocytes over the total number of
to IBD than the mature skeleton. In addition, patients
osteocytes was 3.01% ⫾ 2.23%. None of the parameters
in the study of Ward et al were included at diagnosis,
differed were statistically significant between men and
before treatment had been instituted, which might be a
women with CD.
cause of the difference as well.
Examination of the relationship between bone remod-
The relatively small reduction in bone formation we
eling parameters and osteocyte density as well as osteo-
observed in patients with quiescent CD was also reported
cyte apoptosis did not reveal statistically significant cor-
by Croucher et It must be mentioned that, in con-
relations. Examination of the relationship between
trast to our population, the majority of their patients
disease activity and osteocyte density as well as osteocyte
received prednisolone therapy at time of the bone biopsy.
apoptosis showed a positive correlation of CDAI with the
This is likely to have been a contributory factor to the
percentage of caspase-3–positive osteocytes (r ⫽ 0.496,
bone loss and might explain the stronger reduction in
P ⫽ .022; see ).
bone formation they observed in comparison with ourfindings.
Interestingly, in our study population, a subset of
In this study, bone structure and remodeling in
patients had histomorphometric characteristics resem-
transiliac bone biopsy specimens from patients with qui-
bling osteoporosis rather than osteopenia. In these pa-
escent CD were investigated. In short, our results indicate
tients, all bone formation indices were low and compa-
that trabecular bone volume was lower in patients with
rable to the extent of reduction of bone formation seen
CD than in healthy age- and sex-matched controls. The
by Croucher et al. Because recent corticosteroid treat-
reduction of bone mass was more pronounced in men
ment was an exclusion criterion in this study, current
than in women and was characterized by a reduction in
corticosteroid therapy cannot be the cause of the reduced
trabecular thickness as well as trabecular number. Besides
bone formation in our patients. Sex, age, current medi-
structural differences, we observed a change in bone
cation use, and number of patients with small bowel
remodeling as indicated by a reduced mineral apposition
resection(s) in the past were similar in the subset and
rate in this CD population when compared with healthy
total population. Unfortunately, prospective data on life-
GASTROENTEROLOGY Vol. 140, No. 1
time cumulative dose of glucocorticoids and the history
osteocyte density in bone of patients with CD is within
of number as well as severity of relapses are not available
the range observed in healthy Literature on
in the current study. Both aspects could well be related to
osteocyte apoptosis in healthy controls is limited, be-
a more severely affected bone phenotype. However, a
cause the assessment of apoptotic osteocytes in bone
retrospective estimate showed no statistically significant
specimens is relatively new in bone morphometry. None-
correlation between cumulative glucocorticoid dose and
theless, the percentage of apoptotic osteocytes in our CD
any of the bone formation parameters.
population is comparable to the percentage observed in
Glucocorticoids inhibit differentiation and activity of
hip fracture controls by Sambrook et However, the
osteoblasts and its precursor cells and, moreover, induce
percentage of empty lacunae is relatively high when com-
osteoblast An advantage of this study is that
pared with the controls in that study and resembles more
only patients without recent corticosteroid treatment
the percentage of empty lacunae observed in their pred-
were included. Inherent to this aspect, patients in this
nisone-treated patients with rheumatoid arthritis. This
study were in a quiescent state of disease, which is a
finding may be explained by an increased osteocyte apo-
poorly investigated but interesting group of patients be-
ptosis in the past, because empty lacunae mark sites
cause there are indications that the cumulative effects of
where osteocytes have died previously. This hypothesis is
even small excesses in cytokine levels over many months
corroborated by the positive correlation we observed be-
can be clinically relevant. One of our findings supporting
tween disease activity (CDAI) and the percentage of ap-
this theory is that bone of male patients with CD, who
optotic osteocytes. In that case, osteocyte apoptosis
tended toward longer disease duration, was more severely
might have been increased during an active period of
affected than bone of female patients. Men with CD in
disease in patients with CD. However, C-reactive protein
this cohort had lower bone volume and both less and
level did not correlate with the percentage osteocyte ap-
thinner trabeculae than women with CD. The latter as-
optosis. Because CDAI is inaccurate in the low range, the
pect is in contrast to observations in healthy controls
correlation of CDAI with osteocyte apoptosis might be
describing no difference in bone structure between men
due to chance. Therefore, the biological relevance of this
and Moreover, in postmenopausal popula-
finding remains to be elucidated.
tions, bone loss due to the loss of whole trabeculae has
A drawback of bone histomorphometry is a consider-
been reported mainly in A higher bone turn-
able measurement variation. Differences in staining tech-
over in male patients with CD in this cohort, as indicated
niques, methods to measure the specimen, as well as
by higher levels of alkaline phosphatase than in female
intersection and interobserver variance can be substan-
patients, might partially explain this finding. However,
tial. The number of patients studied is relatively small,
direct differences in bone remodeling indices could not
but it still is the largest series in well-characterized pa-
be detected between men and women with CD, which
tients with IBD. Another limitation is that patients with
suggests the existence of differences between male and
IBD reflect a heterogeneous population. In this study,
female patients in the past.
only patients with CD were included. In addition, these
Bone resorption data were not available in the healthy
patients were in a quiescent state of disease and had not
control population, but when compared with the litera-
used glucocorticoids for at least 3 months before inclu-
ture, osteoclast number and osteoclast surface seemed to
sion. These restrictions to patient inclusion should have
be low in our patients with Our data are in
reduced the impact of heterogeneity in this study. How-
concordance with previous studies addressing bone re-
ever, we still might not have had enough statistical power
sorption in patients with IBD, which showed a slight
to detect certain differences and correlations.
decrease in bone resorption indices in both children and
In conclusion, in this study, for the first time a cohort
adults with These findings raise the question
of adult patients with quiescent CD was evaluated using
whether treatment with antiresorptive agents is beneficial
bone histomorphometry. In these patients, bone mass is
to all patients with CD with osteoporosis or osteopenia.
reduced as characterized by trabecular thinning. Further-
However, additional data on eroded surface, resorption
more, our results show that CD-associated bone loss is
cavities, and serum levels of bone resorption markers are
caused by a reduced bone formation at the tissue level,
necessary to make firm conclusions on bone resorption
possibly as a consequence of decreased osteocyte viability
in this study population.
in the past.
Osteocyte apoptosis interrupts signaling between os-
teocytes and the effector cells of bone: osteoblasts andosteoclasts. Therefore, a lack of osteocytes or inefficacy of
their function can be related to a defective bone structure
1. Bernstein CN, Leslie WD. Review article: osteoporosis and inflam-
and remodeling. As far as we know, osteocyte density and
matory bowel disease. Aliment Pharmacol Ther 2004;19:941–952.
apoptosis in transiliac bone biopsy specimens from pa-
2. Vestergaard P. Bone loss associated with gastrointestinal dis-
tients with CD have not been studied before. From com-
ease: prevalence and pathogenesis. Eur J Gastroenterol Hepatol
parison of our findings with the literature, it appears that
2003;15:851– 856.
BONE HISTOMORPHOMETRY IN QUIESCENT CD
3. Bernstein CN, Leslie WD. The pathophysiology of bone disease in
18. van Essen HW, Holzmann PJ, Blankenstein MA, et al. Effect of
gastrointestinal disease. Eur J Gastroenterol Hepatol 2003;15:
raloxifene treatment on osteocyte apoptosis in postmenopausal
women. Calcif Tissue Int 2007;81:183–190.
4. Moschen AR, Kaser A, Enrich B, et al. The RANKL/OPG system is
19. Lennard-Jones JE. Classification of inflammatory bowel disease.
activated in inflammatory bowel disease and relates to the state
Scand J Gastroenterol Suppl 1989;170:2– 6.
of bone loss. Gut 2005;54:479 – 487.
20. Parfitt AM, Drezner MK, Glorieux FH, et al. Bone histomorphom-
5. Robinson RJ, Iqbal SJ, Abrams K, et al. Increased bone resorption
etry: standardization of nomenclature, symbols, and units. Re-
in patients with Crohn's disease. Aliment Pharmacol Ther 1998;
port of the ASBMR Histomorphometry Nomenclature Committee.
12:699 –705.
J Bone Miner Res 1987;2:595– 610.
6. Dresner-Pollak R, Karmeli F, Eliakim R, et al. Increased urinary
21. Vedi S, Compston JE, Webb A, et al. Histomorphometric analysis
N-telopeptide cross-linked type 1 collagen predicts bone loss in
of bone biopsies from the iliac crest of normal British subjects.
patients with inflammatory bowel disease. Am J Gastroenterol
Metab Bone Dis Relat Res 1982;4:231–236.
2000;95:699 –704.
22. Dalle CL, Bertoldo F, Valenti MT, et al. Histomorphometric anal-
7. Gilman J, Shanahan F, Cashman KD. Altered levels of biochemi-
ysis of glucocorticoid-induced osteoporosis. Micron 2005;36:
cal indices of bone turnover and bone-related vitamins in patients
with Crohn's disease and ulcerative colitis. Aliment Pharmacol
23. Kimmel DB, Recker RR, Gallagher JC, et al. A comparison of iliac
bone histomorphometric data in post-menopausal osteoporotic
8. Abitbol V, Roux C, Chaussade S, et al. Metabolic bone assess-
and normal subjects. Bone Miner 1990;11:217–235.
ment in patients with inflammatory bowel disease. Gastroenter-
24. Ott SM, Oleksik A, Lu Y, et al. Bone histomorphometric and
ology 1995;108:417– 422.
biochemical marker results of a 2-year placebo-controlled trial of
9. Bischoff SC, Herrmann A, Goke M, et al. Altered bone metabolism
raloxifene in postmenopausal women. J Bone Miner Res 2002;
in inflammatory bowel disease. Am J Gastroenterol 1997;92:
25. Sambrook PN, Hughes DR, Nelson AE, et al. Osteocyte viability
10. Bjarnason I, Macpherson A, Mackintosh C, et al. Reduced bone
with glucocorticoid treatment: relation to histomorphometry. Ann
density in patients with inflammatory bowel disease. Gut 1997;
Rheum Dis 2003;62:1215–1217.
40:228 –233.
11. E.F.Eriksen BLMK. The cellular basis of osteoporosis. Spine:
state of the art reviews. 8th ed. 1994.
12. Croucher PI, Vedi S, Motley RJ, et al. Reduced bone formation in
Received June 3, 2010. Accepted September 9, 2010.
patients with osteoporosis associated with inflammatory boweldisease. Osteoporos Int 1993;3:236 –241.
Reprint requests
13. Ward LM, Rauch F, Matzinger MA, et al. Iliac bone histomorphom-
Address requests for reprints to: Nathalie Bravenboer, PhD,
etry in children with newly diagnosed inflammatory bowel dis-
Departments of Endocrinology and Clinical Chemistry, VU University
ease. Osteoporos Int 2010;21:331–337.
Medical Center, PO Box 7057, 1007 MB Amsterdam, The
14. Hessov I, Mosekilde L, Melsen F, et al. Osteopenia with normal
Netherlands. e-mail: fax: (31) 0 20 44 42
vitamin D metabolites after small-bowel resection for Crohn's
disease. Scand J Gastroenterol 1984;19:691– 696.
15. Qiu S, Rao DS, Palnitkar S, et al. Age and distance from the
surface but not menopause reduce osteocyte density in human
The authors thank Prof Dr Juliet Compston and Linda Skingle for
cancellous bone. Bone 2002;31:313–318.
supplying the control material and data.
16. Mullender MG, Tan SD, Vico L, et al. Differences in osteocyte
density and bone histomorphometry between men and women
Conflicts of interest
and between healthy and osteoporotic subjects. Calcif Tissue Int
The authors disclose no conflicts.
17. Qiu S, Rao DS, Palnitkar S, et al. Reduced iliac cancellous
osteocyte density in patients with osteoporotic vertebral fracture.
The Initiative on Crohn and Colitis (ICC) Foundation received a
J Bone Miner Res 2003;18:1657–1663.
research grant from Sanofi-Aventis.
Source: http://icc-ibd.stijlloos.nl/upload/files/publicaties/2011-Oostlander%20et%20al-Gastroenterology.pdf
1. Executive summary2. Business/market background – the challenge for pubs3. The importance of food4. The role of pubs and pub grub5. Pub target audiences6. The opportunity – starters & side orders7. Starters & sides8. Side orders9. Theatre10. The opportunity11. Conclusions Pubs and bars are facing an increasingly tough time as Together with menu familiarity, this means that side orders
For reprint orders, please contact: [email protected] Review 2016/03/29 The germline/soma dichotomy: implications for aging and degenerative disease Human somatic cells are mortal due in large part to telomere shortening associated Michael D West*,1, Francois with cell division. Limited proliferative capacity may, in turn, limit response to injury



