Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Ggh_23_2b.indd
Volume 23 Number 2
Growth, Genetics & Hormones
ISSN 0898-6630 (Print)
ISSN 1932-9032 (Online)
In This Issue
Reviews & Comments
GROWTH IN OSTEOGENESIS IMPERFECTA
Childhood Hypopituitarism
HORACIO PLOTKIN, MD, FAAP
may even be a different degree of severity
24 after Traumatic Brain Injury
Departments of Pediatrics and
in different members of the same family.4,5
Clinical features that may be present
25 Value of Clinical
Radiological Expertise in
University of Nebraska Medical Center
include bone fragility, joint hyperlaxity,
Mutation Screening
and Children's Hospital
muscle weakness, chronic unremitting bone
Omaha, Nebraska
pain, and skul deformities (eg, posterior
26 Height Determinants in
flattening) due to bone fragility in infants
Turner Syndrome – KIGS
with severe OI. Fractures may stil occur
27 Focusing Ilusion: Wealth,
Osteogenesis imperfecta (OI), or brittle bone after puberty,6 with bone fragility persisting
Height, and Happiness
disease, is a rare disorder with congenital throughout life. Individuals with mild forms
bone fragility caused by mutations in the of the disease may have normal stature with
genes that codify for type I pro-col agen no deformities or fractures at al , and the
GH Therapy in Cystic
production in osteoblasts (
COL1A1 and condition would be diagnosed only when
29 Fibrosis
COL1A2), located in chromosomes an x-ray is obtained for other reasons.
MC2R Loss in Salt-losing
7 and 17.1 Numerous mutations have been People with severe OI may have extreme
30 Adrenal Hypoplasia
described as causing the condition.2 In short stature and severe deformity of the
the vast majority of cases, OI is inherited long bones. Exercise tolerance and muscle
30 Mutant IGF-1R as Cause for in a dominant fashion, or caused by a new strength are significantly reduced in patients
Familial Growth Failure
mutation. The prevalence of OI is estimated with OI, even in the mild forms.7
31 Final Height in GHD Patients
to be 1 in 20 000 to 50 000 infants.3
With Normalized Pubertal GH
Osteogenesis imperfecta can affect several
Besides brittle bones, clinical characteristics organs and systems. For example, hearing
E-Reviews & Comments
and severity of OI are widely variable. There loss may be present in about 50% of the
Anorchia and Micropenis in
Infancy and Testosterone Treatment
From The Editor's Desk
Cancer Survivors, GH Treatment
and Second Neoplasms
You may be aware that our former sponsor, Insmed, settled a patent infringement dispute and
CRTAP - Cartilage Deficiency in OI
no longer promotes IGF-I/IGFBP-3 to patients with severe primary IGF-I deficiency or other short
Guidelines for Turner Syndrome
stature indications. Therefore, they no longer provide an educational grant to the GGH journal. Consequently, Pediatric Sunshine Academics, Inc., a 501(c)(3) non-profit organization, is funding
Highlights: International Congress
the cost of this issue of GGH without prior anticipation or alternative funding sources available.
of the GRS and the IGF Society
However, I am committed to seek new grants that wil al ow us to continue publishing this journal.
Leukemia Survivors: GHD, QOL,
I am grateful to the editorial board for their strong support; they have al pledged to contribute with
and Neuropsychological Function
their usual efforts and expertise while we seek more stable times. Since its inception 23 years ago,
Neonatal Dexamethazone,
GGH has improved and expanded; it is held in high regard and enjoys over 11 000 subscribers. We
Growth, and Bone Accretion
al feel obliged not to let you down.
In order to forge ahead GGH wil need the support of its readers while we elicit educational grants. You
Novel FGFR3 Mutations in
can help us during this transition by contributing to Pediatric Sunshine Academics, Inc. an organization whose mission is to support research and education in pediatric endocrinology and nutrition. Your
Prenatal CAH Treatment and
ful y tax deductible donation to
Pediatric Sunshine Academics, Inc., P. O. Box 3208, Tallahassee,
Cognitive Function
FL 32315-3208, either by check or online atwil be used entirely for the
Prepubertal Gynecomastia Linked
continued publication of GGH. Pediatric Sunshine Academics, Inc.'s federal EIN is 65-0854085.
to Lavender and Tea Tree Oils
On behalf of the editorial board, I thank you in advance for your donations and support. I wil
Sleep-related Disturbances in
keep you apprised of our quest to elicit new grants and sponsorships for the continuation of the
Prader-Wil i Syndrome
publication of GGH.
Fima Lifshitz, MD
Stature and Status: Height, Ability,
and Labor Market Outcomes
Where Does the Genome Live?
GGH is supported by an unrestricted educational grant from Pediatric Sunshine Academics, Inc.
GROWTH, GENETICS & HORMONES
individuals with mild forms of OI after the third decade of
very short stature, whereas individuals with type IV OI
life.8 The incidence of congenital malformations of the heart
may have mild-to-moderate short stature. Furthermore,
in children with OI is probably similar to that of the normal
according to some authors, individuals with type IV OI
population,9,10 but respiratory complications secondary to
may have normal stature.21 This highlights the inaccuracy
kyphoscoliosis are common in individuals with severe OI.11
of classifying this disease into 4 types.22 I wil , therefore,
Joint hyperlaxity is also a common occurrence in patients
refer to OI "severity" throughout this article, instead of
with OI,12 and may lead to dislocation of hips and radial
heads, sprains, and flat feet. Constipation and hernias are also a common complication of OI.13 Dentinogenesis
The mean standing height of patients with OI is lower
imperfecta (DI), caused by an abnormal dentin while
than that of their unaffected first degree family members,
enamel remains normal,14,15 is prevalent in about 28% of
regardless of severity. Truncal height is reduced and
OI patients.16 Life expectancy in subjects with non-lethal OI
head size increased in one third of the patients, more
appears to be the same as that in the normal population,17
so in individuals with moderate or severe OI (Sil ence's
with the exception found in cases of very severe OI with
types IV and III). During childhood, there appears to be
respiratory or neurological complications.18
no difference between the standing heights of girls and boys, but women had lower height z-scores than men.
Histomorphometric analysis of the bone in patients with
The reduction in arm span z-score general y fol ows the
OI shows decreased trabecular bone volume, possibly
same pattern as for height: individuals with moderate or
secondary to the formation of fewer trabeculae, and to
severe OI tend to have lower z-scores than individuals
a lack of thickening of trabeculae with growth. There
with mild OI. The arm span/height ratio appears to be
is evidence of defects in modeling of external bone
increased in children with moderate or severe OI, but not
size and shape, production of secondary trabeculae
in those with mild OI. Mean concentrations of insulin-like
by endochondral ossification, and thickening of
growth factor (IGF)-I and IGF binding protein (IGFBP)-3 are
secondary trabeculae by remodeling.19 Contrary to the
general y normal, in the low range of age-specific reference
common conception of attributing the defect in OI to the
values.10,21 Growth hormone (GH) deficiency is very rare in
osteoclast, OI should be regarded as a disease of the
patients with OI. In a group of 22 children tested by Marini
osteoblast. Col agen plays an essential role in forming
et al,23 none fulfil ed the standard criteria for GH deficiency.
an interactive network between the cel s by making
A few children in that study had a blunted response to
extracel ular matrix and noncollagenous proteins that
GH-releasing hormone or failed to double their serum IGF-I
lead to proper mineralization of the bone. When the
in a 5-day somatomedin generation test. However, there
fundamental structure of the col agen helix is disturbed
was no consistent relationship between those responses
by a mutation, a complex series of secondary changes to
or between the responses and type of OI.
the bone develops, leading to increased bone fragility.
The etiology of the growth restriction in children with
GROWTH IN CHILDREN WITH OI
moderate and severe OI is not entirely clear. It has been
Severely affected patients may be short because of
suggested that it could be viewed as a self-protective
vertebral compression fractures, severe scoliosis, lower
mechanism: a given mechanical load creates smal er
limb deformities, and disruption of growth plates.20
stresses in a short bone than in a long bone, thus a short
However, growth can also be delayed in the absence
bone wil break less easily.24 People with severe OI have
of these abnormalities. The most commonly used
a typical deformity of the growth cartilage, defined as
classification divides OI into 4 types. Type I patients
"popcorn" appearance of the metaphysis. Microfractures
do not have bone deformities and may have normal
of the growth cartilage may play a role in the growth
height, but fractures may range from very few to dozens
problems experienced by these patients. There are no
over a lifetime. Type II is the most severe, with patients
reports on the effects of puberty and hormonal changes
usually not surviving the perinatal period. Patients with
on growth in children with OI.
type III have a characteristic triangular face, very short stature, and severe bowing of long bones; they typically
USE OF BISPHOSPHONATES IN CHILDREN WITH OI
suffer many fractures throughout their life. Type IV is not
Bisphosphonates are synthetic drugs with a chemical
clearly defined. Patients with this type of OI are general y
structure based on pyrophosphate,25 and have been used
short, although there is no consensus regarding the
to treat osteopenia of primary and secondary origin in
specific characteristics of this type. Other types have
both children and adults.26 Effects on both osteoblasts27,28
been described, but there is controversy because they
and osteoclasts29,30 have been shown, although the
actual y represent syndromes resembling OI.1 According
mechanism through which bisphosphonates increase
to one study, during the first 10 years of life the number
bone mineral density (BMD) is not clear (Figure 1).
of fractures, extent of skeletal deformities, and growth
Likewise, effects of bisphosphonates on growth
retardation do not differ between OI types III and IV.10 This
have been documented, but the mechanism of those
is surprising, as individuals with type III OI usually have
effects has not been elucidated. There are differences
18
GGH Vol. 23, No. 2 June 2007
GROWTH, GENETICS & HORMONES
decreases as wel . Fracture healing does not appear
Increase osteoclast apoptosis?
Decrease osteoblast apoptosis
to be impaired in patients with OI when compared to untreated OI patients.37,38 There is a striking disappearance of bone pain and decreased fracture
incidence noted with intravenous treatment. This
may contribute to greater mobility,39,40 an essential factor for the development of the skeletal system.41
A lower fracture incidence, despite higher risk of
injury due to increased mobility, suggests a direct effect of the therapy. These effects contribute to an
improvement in the quality of life of patients with OI
who are receiving treatment.
A side effect of high doses of pamidronate (9 mg/kg/yr) is retention of calcified cartilage within
Interfere with osteoclast function?
secondary spongiosa in children with OI.30 Higher
Figure 1. Possible mechanisms of action of bisphosphonates on bone.
doses have caused osteopetrosis in a patient with no diagnosis.42 Retention of calcified cartilage within
among the bisphosphonates that may influence their
secondary spongiosa is a hal mark of osteopetrosis,
mechanisms for binding and inhibiting bone crystal
this suggests a dose-related effect of pamidronate.
growth and dissolution. This may explain differences
Studies using oral bisphosphonates for the treatment of
in potency among different bisphosphonates, such as
OI (olpadronate,43 alendronate) showed no differences
the apparently more prolonged duration of action of
between the drugs and placebo on functional outcome,
alendronate and zoledronic acid, compared with the more
anthropometrics, fracture incidence, or vertebral height,
readily reversible effects of risedronate.31
although it has been suggested that oral alendronate may improve quality of life in this group of patients.44
Different treatment protocols recommend the use of different bisphosphonates (ie, pamidronate, risedronate,
EFFECTS OF BISPHOSPHONATE TREATMENT ON
alendronate, olpadronate, neridronate), and at different
GROWTH IN CHILDREN WITH OI
dose regimens for the pediatric population. For example,
The effect of treatment with bisphosphonates on
pamidronate doses range from 4.5 mg/kg/yr32,33 (Tables 1
longitudinal bone growth in children has been a concern
and 2) to 9 mg/kg/yr.34,35 Children treated with high-dose
among clinicians.45 Bone resorption is an essential part
pamidronate experience dramatic increase in BMD, with
of the normal endochondral ossification process,46
changes of as high as 200% per year.35,36 Other positive
and of the bone modeling and remodeling process.
effects observed include increase of the cortical width
Despite the fact that the mechanism of long bone
of the metacarpals, and increased vertebral height in
growth relies upon clonal expansion and subsequent
previously fractured vertebrae. The incidence of fractures
hypertrophy of chondrocytes, endochondral bone growth requires resorption of the septa of calcified cartilage at the chondro-osseous junction of the growth plate
Table 1. Protocol for administration of low-dose IV
by chondroclasts, permitting vascular invasion of the
hypertrophic cell lacunae.47 Drugs interfering with this
Age group
mechanism could potentially cause impairment of the
0.37 mg/kg/day for 2 days
bone elongation process. Bisphosphonates interfere with osteoclast function29 or survival,48 and could, therefore,
0.56 mg/kg/day for 2 days
have a deleterious effect on bone growth. This undesired
0.75 mg/kg/day for 2 days
effect has actually been shown in animal studies.49 High doses of alendronate (>2.5 mg/kg/wk) inhibited long bone length in the OIM mice (a model of OI) through alteration
Table 2. Suggested dilution and infusion rates for IV
of the growth plate and possibly reduced resorption at the chondro-osseous junction.50 Furthermore, lower
mg of pamidronate
mL of normal saline
doses of alendronate do not appear to have a detrimental
effect on growth in oim/oim mice,51 suggesting another
dose-related effect of bisphosphonates. On the other
hand, bisphosphonates do not appear to be detrimental
for growth in human subjects at the doses currently used (Figure 2).24,52-55 Each time a patient receives a
pamidronate infusion, a new sclerotic line appears in the
GGH Vol. 23, No. 2 June 2007 19



GROWTH, GENETICS & HORMONES
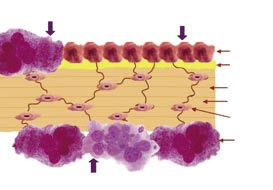
Figure 2. Lower limbs x-ray of a child with severe OI before (a) and after 12 months (b) of treatment with low-dose pamidronate
(4.5 mg/kg/yr). Treatment was started at 18 months of age. Note longitudinal growth. Fractures do occur under treatment as evident in the
panel on the right, but at much lower rate than before treatment.
metaphysis of long bones. The distance between these
in those with more severe forms of the condition when
lines reflects longitudinal bone growth (Figure 3).
receiving therapy with alendronate or pamidronate.57
Pamidronate in high doses (9 mg/kg/yr) does not appear
One study showed that patients treated with high doses of
to negatively affect growth. Height z-score actually
pamidronate (9 mg/kg/yr) had similar growth plate width but
increased in a group of patients
wider metaphyses when compared with
with OI who had started treatment
untreated OI patients who were matched
before 3 years of age.35 After one
for OI type and age, despite the lack of
year of pamidronate therapy, height
detrimental effects of bisphosphonates
z-scores increased significantly in a
on longitudinal growth,58 suggesting
group of children with severe OI and
an effect of the high dose on bone
did not change in children with mild
remodeling. A different study showed
and moderate OI.24 After 4 years of
that metaphyseal modeling in the
therapy with the same dose regimen
distal femur is constant in children on
of pamidronate, mean height z-scores
bisphosphonates—with slight variation
increased significantly in children with
between sexes—resulting in a similar
moderate OI, whereas non-significant
shape of the distal femur throughout
trends to increase were seen in
childhood when looking at the modeling
patients with mild and severe OI.24
process.59 Noteworthy, the observed
Low doses of pamidronate appear
positive effect of pamidronate on bone
to have a similar effect (data not
growth does not appear to be secondary
published) (Figure 3).
to acceleration of bone age.24
Low doses of pamidronate elicited
Infants with OI appear to grow better
no short-term evidence of growth
when treatment with neridronate is
impairment in children with a variety of
started soon after birth, rather than at
pathologies leading to osteoporosis,
6 months of age.60 Older children with
including OI. A median annualized Figure 3. Distal femur of a pediatric OI receiving neridronate grew faster
change in height SDS of 0 (range, patient with OI receiving treatment with than controls in one study.61 At the
–0.4 to 0.5) was noted in that group.56 IV pamidronate. Note the sclerotic lines, microscopic level, the size of iliac crest
each representing an infusion. The distance
As expected, growth changes are between lines reflects longitudinal bone bone biopsies is not significantly different
greater in children with milder OI than growth in a 2-month period.
before or after treatment in children
20 GGH Vol. 23, No. 2 June 2007



GROWTH, GENETICS & HORMONES
with OI. Changes are seen in cortical
in patients with moderate OI, and
width, which increased by about 90%.
9 cm in patients with severe OI
Cancel ous bone volume increases
can be expected at 15 years of
by about 45% with treatment. This
age. These results suggest that
change is due to higher trabecular
acceleration of growth is not just a
number, with no change in trabecular
transitory effect, but rather a lasting
thickness.30 Importantly, there is no
outcome on height in children with
evidence for a mineralization defect
OI who are receiving pamidronate
in children with OI treated with high
intravenously. As mentioned
doses of pamidronate.30 Growth in
above, it is not entirely clear how
children continues after treatment
pamidronate treatment might
with pamidronate is stopped, and the
improve growth. Part of the effects
newly-formed bone wil be unprotected
of bisphosphonates on growth in
and prone to fractures (Figure 4).
children with moderate and severe OI could be due to prevention of long
LONG-TERM EFFECTS OF
bone deformity and regeneration of
BISPHOSPHONATES ON HEIGHT
vertebral fractures (Figure 5),35,62
In one study, mean height z-scores
and to prevention of microfractures
of subjects with all OI degrees of
affecting growth cartilage.
severity tended to increase after 4 years of pamidronate therapy when
EFFECTS OF GROWTH
compared with baseline. However,
HORMONE IN CHILDREN WITH OI
the change in height z-scores was
Growth hormone regulates post-
significant only for the group with Figure 4. Long bones continue growing after natal bone growth; IGF-I mediates
moderate OI, but not for mild or treatment with bisphosphonates is stopped the growth-promoting action of GH,
(arrow), causing susceptibility to fractures.
severe OI.24 It is of note that these
although it has been shown that
comparisons were done against normal growth charts
GH may have independent, direct effects on growth.63
designed for healthy children. To more accurately
Also, IGF-I has mitogenic effects in dividing cells and
assess the growth rate of children with OI undergoing
is closely associated with growth, although plasma
treatment, the same group compared their growth with
levels do not correlate with growth rates. It is known to
that of a group of children with OI who were not receiving treatment with bisphosphonates. In that study, each height measurement of patients was expressed as a percentage of the mean value expected for untreated OI patients. During 4 years of pamidronate therapy, height significantly increased above the values expected for untreated patients.24
EFFECT OF PAMIDRONATE
ON FINAL HEIGHT
There is very little information
about final height in children with
OI treated with bisphosphonates.
There is the description of only
8 patients who attained final height
while receiving treatment with
pamidronate.24 In this study, final
height, expressed as a percentage
of the expected height in untreated
patients, was significantly higher than baseline height. This study
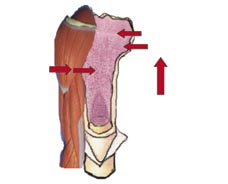
Figure 5. Lumbar spine x-ray of a child with severe OI before (a) and after 12 months (b) of
suggests that an average gain of
treatment with low-dose pamidronate (4.5 mg/kg/yr). Treatment was started at 18 months of
7 cm in patients with mild OI, 12 cm
age. Note increased vertebral height with treatment.
GGH Vol. 23, No. 2 June 2007 21
GROWTH, GENETICS & HORMONES
increase 1-α hydroxylase in kidneys, with subsequent
and the largest bone strains, and those strains help to
increased production of calcitriol (1,25 [OH]2 vitamin
control the biological mechanisms that determine whole-
D3). As calcitriol is the active form of vitamin D, IGF-I and
bone strength (Figure 6).72
GH treatment can make calcium more available for bone mineralization,64 which could add to a possible beneficial
There are no large control ed studies of GH treatment in
effect in patients with OI. Inversely, it has been suggested
children with OI. Furthermore, there are no data in the
that vitamin D, calcium, and protein supplements
literature regarding final height in OI patients treated with
may elicit part of their effect on osteoporosis through
GH. An increase of fracture rate during GH therapy has
increased IGF-I levels.65
been reported in children with OI by different groups,73,74 although another group did not find an increase in fracture
IGF-I promotes longitudinal bone growth by ‘insulin-
rate in a smal group of children with mild OI who were
like' anabolic actions which augment chondrocyte
treated with GH for 1 year.75 Extending treatment to 2 years
hypertrophy.66 Chondrocyte differentiation, in turn, leads
did not change the fracture risk either.76 Like al children
to cartilage expansion and linear growth. Furthermore,
who are initial y started on GH, children with OI experience
osteoblasts and pre-osteoblasts secrete IGF-I, and
an initial acceleration of growth rate,64,77 but a sustained
bone resorption causes release of stored IGF-I. This
effect has not been demonstrated. In one study, GH
hormone appears to be a growth factor for osteoblasts. A
(0.1- 0.2 IU/kg/d for 6 days/wk) was administrated for at
homozygous molecular defect in the gene encoding IGF-I
least 1 year to children with OI of different severity;78 about
caused severe intrauterine growth failure, sensorineural
one-half of the treated OI children sustained a 50% or
deafness, and mild mental retardation in one individual.67
more increase in linear growth, compared to their baseline
Treatment with IGF-I improved linear growth and insulin
growth rate. It is of note that most responders (10 of 14) did
sensitivity in that patient.68 There is also some weak
not have a severe form of OI. Incidental y, only the linear
evidence that IGF-I has a role in declining BMD with
growth responders had a significant decrease in long
aging. In patients with Laron syndrome, IGF-I treatment
bone fractures. After 1 year of treatment, responders' iliac
increases bone growth in the absence of GH.69 Low IGF-I
crest biopsy showed significant increases in cancel ous
concentrations appear to be associated with low BMD
bone volume, trabecular number, and bone formation
in patients with cystic fibrosis.70
rate, but no significant increase in cortical thickness. Histomorphometric parameters of bone resorption were
As discussed above, some children with OI have a blunted
not significantly changed in responders, whereas non-
response to GH-releasing hormone or fail to double their
responders had an 80% increase in the percentage of
serum IGF-I in a 5-day somatomedin generation test (13
bone surface covered by osteoclasts. The incidence
of 22 had less than a 2-fold stimulation of somatomedin-C
of fractures was unchanged in non-responders. Bone
by GH).71 There was no overlap between the group with
formation parameters did not increase with treatment
blunted IGF-I response and the group with decreased GH-
in this group. Although progression of scoliosis was
releasing hormone response, suggesting that there might
unchanged compared with the National Institute of Child
be 2 different mechanisms of GH resistance in children
Health and Human Development (NICHD) OI population,
with OI. GH is an anabolic hormone and, together with
data on individual cases are not offered in the report.
IGF-I, is a potent regulator of muscle mass. As such, there is potential for it to increase bone density. In the absence
Recombinant human IGF-I, complexed with its
of trauma, muscles are responsible for the largest loads
predominant binding protein IGFBP-3 is currently being tested as a treatment for osteoporosis, alone or in combination with anti-resorptive drugs and GH.79 There appears to be a correlation between the dose of GH (and
Direct action on growth
the obtained IGF-I plasma levels) and the increase in
bone turnover markers and/or BMD in adults,80 although
Increases
a different study found that 1 year of IGF-I treatment, at
a dose sufficient to elevate circulating IGF-I to young
normal values, was not an effective means to alter body composition or blood parameters, nor to improve bone
Increases Igf-I secretion
density, strength, mood, or memory in older women.81
CONCLUSION
Bisphosphonate treatment does not appear to have
a detrimental effect on linear growth in children and
adolescents with OI, regardless of the severity of the
condition. Long-term bisphosphonate therapy in children
Figure 6. Mechanisms for growth hormone stimulation of bone
with OI may be associated with a significant height gain,
growth and increase of bone mineral density.
as compared with untreated OI patients with the same
22 GGH Vol. 23, No. 2 June 2007
GROWTH, GENETICS & HORMONES
disease severity. The use of GH in this population is stil
controversial. It has been suggested that GH treatment
should probably not be used as a first-line therapy in OI.82
Combined protocols administering both bisphosphonates
39. Plotkin H, Gibis J, Glorieux FH. Bone. 2001;28:S78.
and GH are warranted. Other therapeutic options currently
used or in research for patients with osteoporosis (PTH,
IGF-I, strontium, RANK ligand) may have a role in the
treatment of OI in the future.
Disclosures: The author discloses no conflicts of interest. Pamidronate
use for children with OI is off label.
46. Ross FP. Osteoclast biology and bone resorption. In: Favus MJ, ed.
Primer on the Metabolic Bone Diseases and Disorders of Mineral
Metabolism. 6 ed. Washington, DC: ASBMR; 2006:30-5.
20. Plotkin H. Syndromes with brittle bones, hyperostotic bone diseases
66. Jie W, Jian Z, Bondy C. FASEB J. 1999;13:1985-90.
and fibrous dysplasia of bone. In: Lifshitz F, ed. Pediatric Endocrinology.
Vol 2, 5th edition. New York, NY: Informa;2007:559-70.
73. Kinugasa A, Fujita K, Inoue F, et al. Acta Ped Scan.
76. Antoniazzi F. Therapeutic approach with growth hormone. In: 7th
International Conference on Osteogenesis Imperfecta. Montreal,
Canada; 1999:1-16.
36. Munns CF, Rauch F, Travers R, et al. J Bone Miner Res.
GGH Vol. 23, No. 2 June 2007 23
Source: http://www.osteogenesis.info/almacen/growth.pdf
Federal Agency Name: United States Agency for International (USAID) Mission to Ethiopia Funding Opportunity Title: TRANSFORM/Primary Health Care Unit (TRANSFOR/PHCU) Announcement Type: Annual Program Statement (APS) Notice of Funding Opportunity Number: APS-663-16-000005 Catalog of Federal Domestic Assistance (CFDA) Number:
Kno c he nmarke rkrankung e n Priv.-Do z. Dr. Ro land Re pp Me dizinis c he Klinik V Klinikum Bambe rg Was will ic h Ihne n e rzähle n … • Funktion des Knochenmarks • Welche Symptome werden durch ein gestörtes Knochenmark verursacht? • Was sind die häufigsten Erkrankungen des Knochenmarks? • Wie werden diese Erkrankungen



