Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Iranjradiol.com
Iran J Radiol. 2014 May; 11(2): e16327.
Published online 2014 May 15.
The Role of Choice-Lock Catheter and Trocar Technique in Percutaneous
Ablation of Symptomatic Renal Cysts
Burak Ozkan 1,*; Ali Harman 1; Baris Emiroglu 1; Ilker Arer 1; Cuneyt Aytekin 11Department of Interventional Radiology, School of Medicine, Baskent University, Besevler, Turkey
*Corresponding author: Burak Ozkan, Department of Interventional Radiology, School of Medicine, Baskent University, Besevler, Turkey. Tel: +90-5056384753, Fax: +90-3124820575,
Received: August 3, 2013
; Revised: December 13, 2013
; Accepted: February 9, 2014
Background: The most common benign lesions of the kidney are simple cysts. They are acquired lesions and mostly affect the elderly
Objectives: To describe the usage of choice-lock catheter and trocar technique in percutaneous renal cyst treatment and determining
long-term outcomes.
Patients and Methods: This retrospective study was carried out between February 2000 and July 2011. Eighty-eight cysts all of which were
Bosniak type-1 cysts were selected in 75 patients. The treatment indications were flank pain, hydronephrosis and hypertension. The choice-
lock catheter was used for 84 cysts with the trocar technique. Ninety-five percent ethanol was used as the sclerosing agent. Maximum
volume of the injected ethanol was 175 ml. The mean follow-up time after the treatment procedure was 23 months. Sixty-four cysts were
located in the cortical and 24 cysts were located at the parapelvic region.
Results: Fifty-seven cysts had complete regression, while 31 cysts regressed partially. After the procedure, pain was relieved in 44 (82%)
patients and the pain alleviated in four (8%). Normotension was obtained in five (62.5%) of the eight hypertensive patients and no
hydronephrosis was detected in nine patients. There were no relationship between the localization and the regression rate. No major
Conclusions: Percutaneous ethanol sclerotheraphy in simple cysts is a safe, cost-effective and minimally invasive method. We consider
that this technique may be an alternative solution in the percutaneous cyst treatment.
Keywords: Simple Renal Cysts; Percutaneous Cyst Ablation; Ethanol Sclerotherapy; Choice-Lock Catheter; Trocar Technique
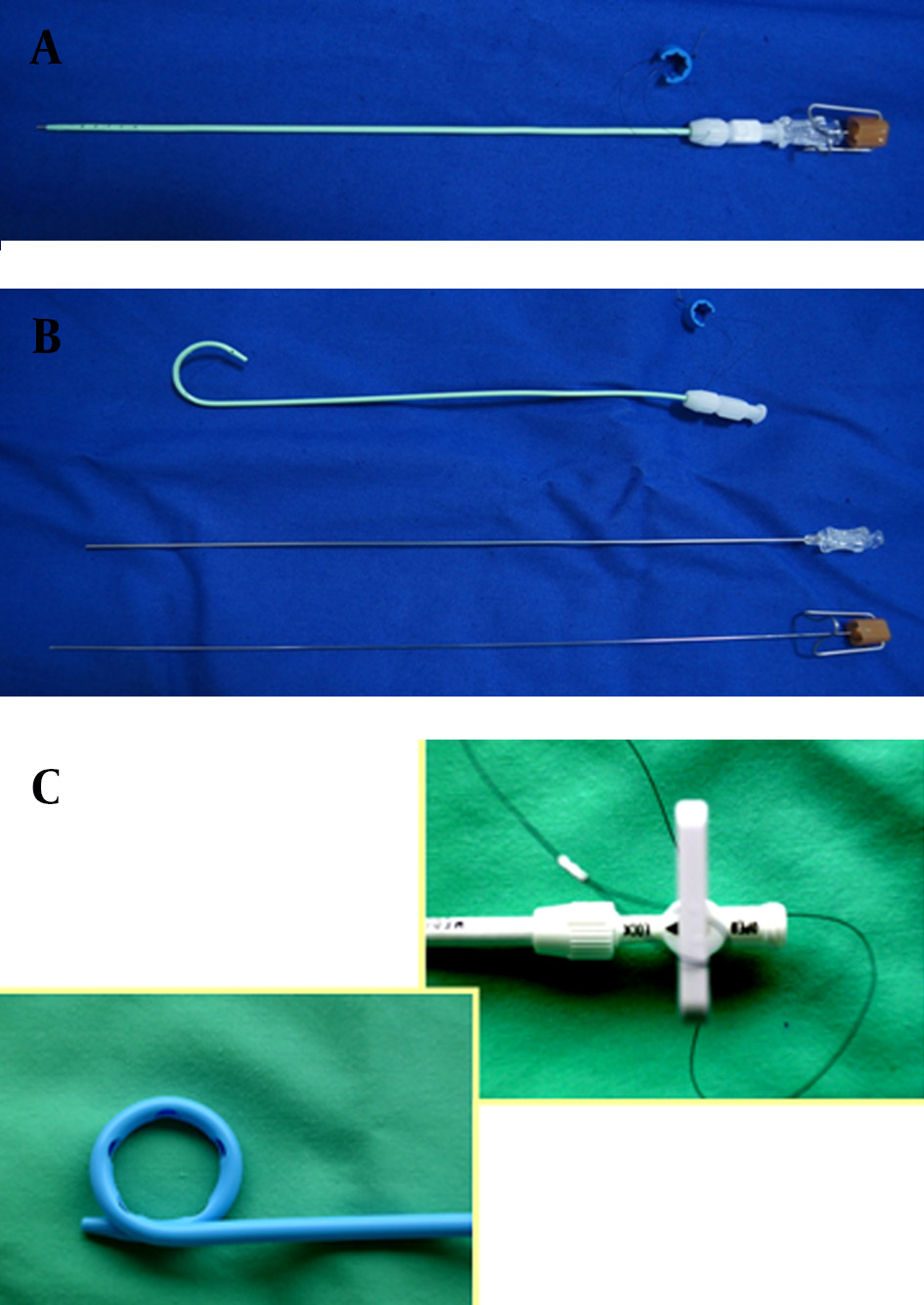
catheters are over 6 French sized. Choice-lock catheter con-
The most common benign lesions of the kidney are the
sists of three co-axial parts. The stillet, the most inner part
simple cysts. They are acquired lesions that mostly affect
of the catheter can also be used for the initial puncture
the elderly population (1). The incidence of the simple
site. This catheter has a special lockage system that enables
renal cyst is more than 50% at age of 50 years. The renal
the catheter stability of the trocar during the puncture
cysts occur by weakening of the epithelium of the collect-
with one hand usage. There is a metal cannula for support-
ing duct cells leading to the diverticula formation pro-
ive aim between the pigtail plastic catheter and the stillet.
cess by time (2). The indication for treatment is based on
The supportive metallic part of the catheter is located in
urinary tract obstruction. Several methods for treatment
the catheter, it stables the other parts to be guided. This
of the cyst including surgical and percutaneous proce-
option enables the catheter to be guided safely through-
dures have been proposed; namely, percutaneous mar-
out the hardened tissues. At the most outer part, there is
supialization (3), percutaneous aspiration (4), and open
a hydrophilic covered plastic part that has a pigtail lock-
and laparoscopic cyst unroofing (5). Aspiration alone
age system (Figure 1). The catheter can be used instead by
without injection of a sclerosing agent has been reported
the Seldinger technique with the help of 0.018 inch guide
with a higher recurrence rate. There are several promis-
ing results with single or multi-session sclerotherapy
with percutaneous drainage (6, 7).
The advantage of choice-lock catheter is the 5.7 F diam-
The aim of this study was to assess the role of choice-
eter. The diameter of the choice-lock catheter is smaller
lock catheter and trocar technique in percutaneous renal
than other draining catheters. Moreover, other draining
cyst treatment.
Implication for health policy/practice/research/medical education:
This paper gives rise to the minimally invasive treatment options in Bosniak cyst treatment.
Copyright 2014, Tehran University of Medical Sciences and Iranian Society of Radiology; Published by Kowsar Corp. This is an open-access article distributed under
the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work
is properly cited.
Ozkan B et al.
were septated and aspiration did not yield acceptable
treatment results at the first attempt. In these patients,
the choice-lock catheter was replaced by 8F pigtail cath-
eter without doing a new puncture. In these cases, sub-
sequently, the 6F dilatator was replaced by the puncture
site with the guidance of 0.018 inch wire that was inside
the choice-lock catheter. The 8 F pigtail catheter (Flexima,
APDL, Boston Scientific, USA) was inserted into the cavity
over a 0.035 inch guide wire (Amplatz stiff guide wire,
Boston Scientific, USA). Twenty milliliter of the fluid was
aspirated from the cavity with the help of the needle. The
fluid was checked for further examinations. To obtain
the cystogram under fluoroscopy, 50% diluted Telebrix
(350 mg iodine/mL, Guerbet, France) was used. The aim
of the cystogram is to assess the relationship of the cyst
with the collecting system and to determine Bosniak
classification. Without any extravasation or communi-
cation with the collecting system, the cyst volume was
aspirated. Equal to 30% of the initial cyst volume of 95%
ethanol was injected into the cavity under fluoroscopic
guidance. The patient was checked for any compliance of
pain or other related symptoms--if the patient tolerated
the session well, 95% ethanol was left in the cavity for 15
minutes. The patient was placed in at least three supine,
prone and both lateral decubital positions. The reason
was to allow contact of ethanol with all the cyst's walls in
order to destroy the epithelial tissue of the renal cyst. At
the end of the procedure, all the injected ethanol to the
cavity was aspirated and the catheter was withdrawn. The
Figure 1. The structure of choice-lock catheter; A) The straight structure
patients were called for periodic ultrasound and/or CT ex-
of the choice-lock catheter; B) The three co-axial parts of the choice-lock
aminations at several follow-up times. The patients were
catheter; C) The specific lockage system of the choice-lock catheter
questioned about the symptoms and the volume of the
treated cysts was calculated. The mean follow-up period
was 23 months ranging from 3 to 58 months. Forty-two
3. Patients and Methods
patients were followed for at least 2 years or more (29 pa-
This retrospective study consisted of 132 patients with
tients had 2, six patients had 3, five patients had 4, and
138 simple renal cysts who underwent percutaneous two patients had 6 years follow-up).
sclerotherapy and ethanol ablation treatment between
SPSS for Windows Ver 11.5 (SPSS Inc., Chicago, Ill, USA)
February 2000 and July 2011 in our clinic. Fifty-seven pa-
was used for statistical analysis. The Shapiro-Wilk test
tients were excluded from the study due to lack of suffi-
was used to determine if the distribution of the continu-
cient clinical data especially follow-up data. Most of these
ous variables were normal. The descriptive statistics for
patients were referred to our clinic from another hospi-
continuous variables were defined as mean±standard
tal. Seventy-five patients with 88 cysts had initial criteria
deviation or median (min-max). For the categorical vari-
for the study. Forty-two patients were male and 33 were
ables, the percent of patients and variables was calculat-
female. The mean age of the patients was 64 years (range,
ed. The Wilcoxon sign rank test was used for evaluation
44-87 years). The patients who underwent percutaneous
if there was a statistically significant change in the cyst
treatment had only type I Bosniak cysts (8). Sclerother-
volume before and after treatment. P value less than 0.05
apy indications included flank pain in 58 (77%), hydro-
was considered statistically significant. The Hospital Re-
nephrosis in nine (10%), and hypertension in eight (9%)
search Ethic Committee approved the study protocol.
patients. The initial criteria for success after treatment
was 60% volume reduction of the cyst. Sixty to eighty
4. Results
percent reduction of the cyst volume was considered as
Between February 2000 and June 2011, 88 cysts among
partial regression, and more than 80% was considered as
75 patients who had percutaneous cyst aspiration and
complete regression. The choice-lock 5.7 F catheter with
ethanol sclerotherapy were evaluated. Eighty-four cysts
trocar technique is used for percutaneous cyst treatment
were treated with choice-lock with trocar technique. In
and ethanol sclerotherapy. In four patients, the cysts
four patients, the cysts were septated and aspiration did
Iran J Radiol. 2014;11(2):e16327
Ozkan B et al.
not yield acceptable results without performing a new
and 2). A total of 75 patients who underwent percutaneous
puncture; therefore, choice-lock catheter was changed
aspiration and sclerotherapy had no major complications
with 8F pigtail catheter under fluoroscopic or sono-
such as renal parenchymal injury, renovascular or renal
graphic guidance. All catheterization procedures were
collecting system injury, pneumothorax or mortality. Pa-
technically successful. The mean volume of the cyst be-
tients using ethanol during sclerotherapy can have minor
fore treatment was 145.65 mL (39-504 mL) and it reached
complications such as allergic reaction, microscopic he-
15.5 mL (0-126 mL) after treatment (P<0.001). After the
maturia or infection. Depending on the amount of etha-
procedure, 57 cysts showed a higher than 80% volume
nol used during sclerotherapy patients may develop tran-
reduction and 31 cysts had 60-80% volume reduction.
sient pain and this is the restriction of ethanol usage. This
None of the patients had any malignant cells in the cy-
is usually related with ethanol extravasation. No patient
had retroperitoneal hemorrhage or hemorrhage into the
Sixty-four cysts were located in the cortical and 24 cysts
were located at the parapelvic region. Before starting the
cyst cavity.
procedure, the median value of the cyst was 174.8 mL (49-
Symptoms (flank pain, hydronephrosis and hyperten-
504) ml in the cortical group, and 85 ml (36-175 mL) in the
sion) resolved in 66 (88%) of 75 symptomatic patients.
parapelvic group. After the procedure, the median value of
Forty-eight (83%) of 58 patients with pain responded well
the cyst volume was 17.3 mL (0.00-105 mL) in the cortical re-
to the treatment. Forty-four (76%) were free of pain, in
gion group, and 6.8 ml (0-65 mL) in the parapelvic located
four (6%) patients the pain decreased, whereas in four
group. There was no statistically significant difference in
(6%) patients the pain did not change, and in six (10%) pa-
the rate of regression between cortical and parapelvic lo-
tients, the pain increased. The patients' symptoms before
cated cysts (P=0.892). There was no statistically significant
and after effective sclerotherapy are mentioned in Table
difference in the rate of regression between two genders
3. The successful treatment of a renal cyst is shown in Fig-
and two groups of small and large volume cysts (Tables 1
ure 2 and Figure 3.
Table 1. Mean Volume of the Cysts Before and After Treatment in Two Genders
Number of Patients (n = 75) Number of Cysts (n = 88)
The Mean Volume of the
The Mean Volume of the
Cysts Before Treatment, cc
Cysts After Treatment, cc
Table 2. Mean Volume of the Cysts Before and After Treatment in Two Groups of Large and Small Cysts
The Mean Volume of the Cysts Before The Mean Volume of the Cysts After
Cysts Larger than 300 cc (n = 20)
Cysts Smaller than 300 cc (n = 68)
128.65 (39.6-294 )
Table 3. Patients' Symptoms Before and After Effective Sclerotherapy
Number of Patients Who Described Symptoms
Number of Patients Whose Symptoms Resolved
Before Effective Sclerotherapy
After Effective Sclerotherapy
Flank Pain
Iran J Radiol. 2014;11(2):e16327
Ozkan B et al.
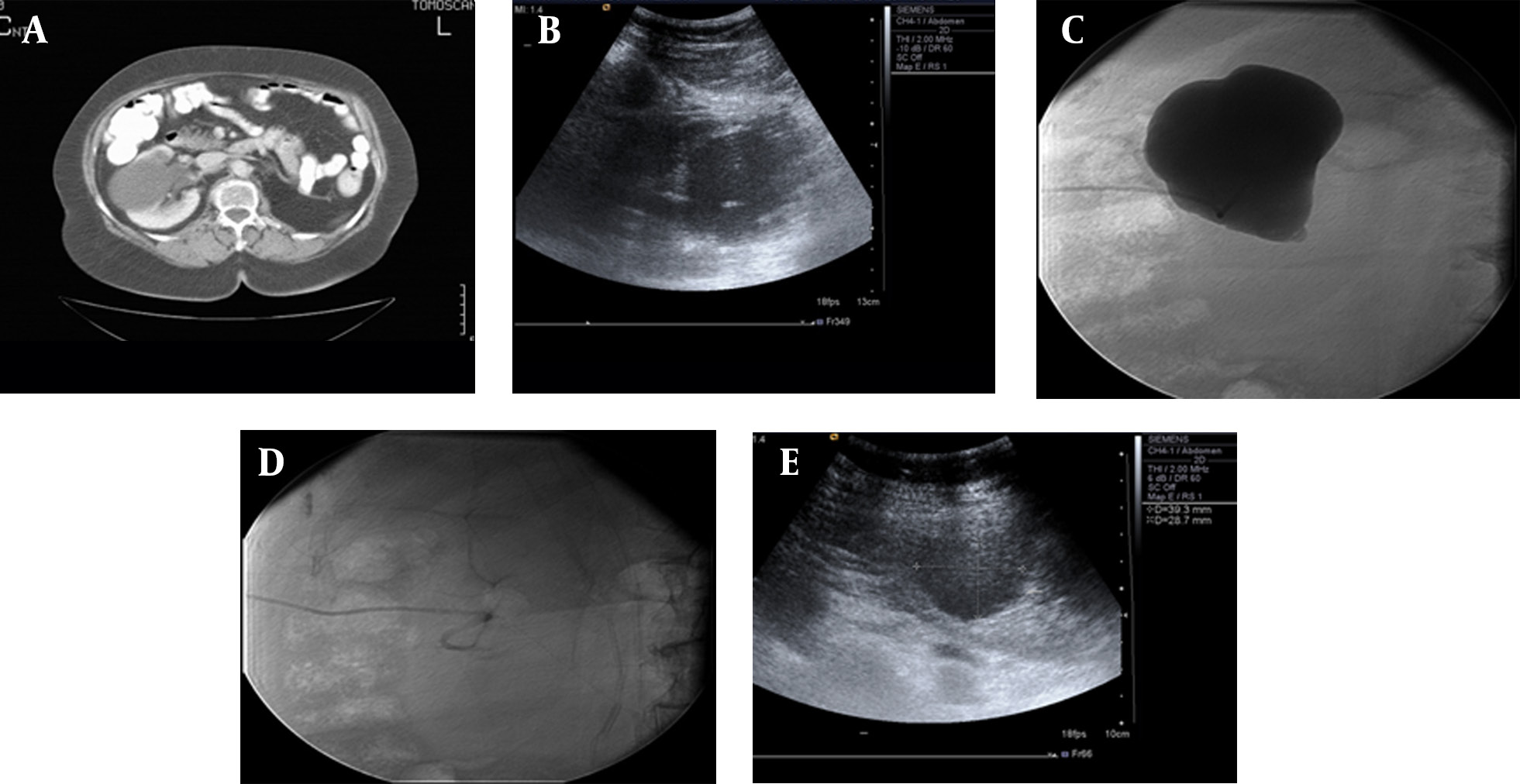
Figure 2. A 56-year-old man with Bosniak type-1 cyst in the right kidney with flank pain. A) Axial CT image shows Bosniak type-1 cyst in the right kidney
which has affected the pelvicalyceal system; B) US image shows the initial catheterization of the choice-lock catheter in the cyst during the treatment
procedure; C) Cystogram shows that the cyst does not have any relationship with the pelvicalyceal system; D) Cystogram obtained after emptying of the
cystic fluid; E) US image shows partial regression of the cyst one month after treatment.
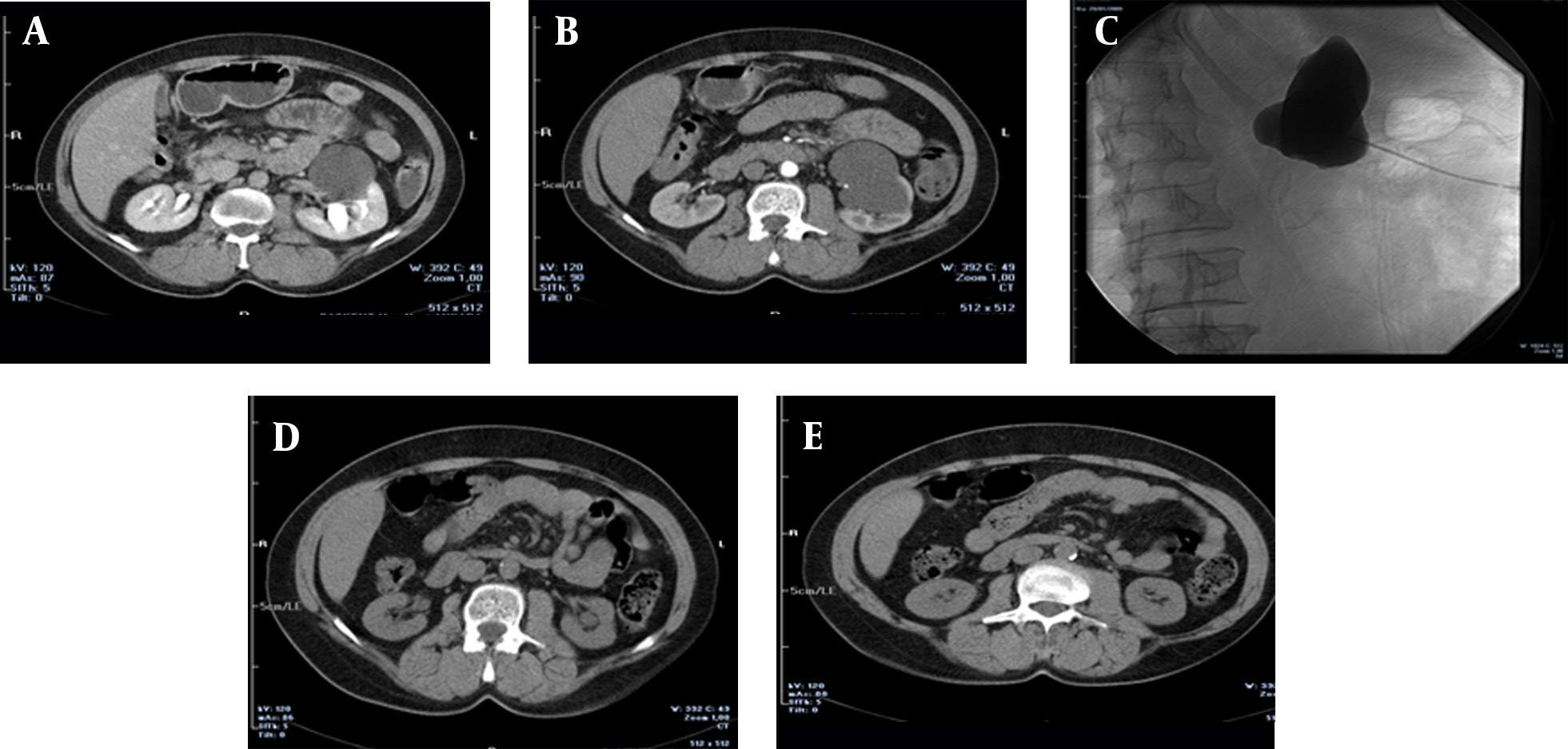
Figure 3. A 72-year-old man suffering from left flank pain for 6 months, A and B) IV contrast enhanced CT images show the cyst located at the lower portion
of the left kidney which is classified at Bosniak type-1; C) Cystogram image shows that the cyst does not connect with the pelvicalyceal system; D and E) CT
images obtained 3 months after the treatment show that the cyst is completely regressed and the patient had no pain.
Percutaneous aspiration and sclerotherapy is the first-
minimally invasive procedure. Simple drainage without
line treatment option for symptomatic simple renal sclerotherapy is associated with a high recurrence rate
cysts (1). Percutaneous aspiration is a simple, safe and
of 40-80%. Percutaneous sclerotherapy using a sclerosing
Iran J Radiol. 2014;11(2):e16327
Ozkan B et al.
agent provides more satisfactory results than aspiration
sclerotherapy with ethanol depends on the injection by
alone (2). In aspiration alone, the destruction of epithe-
increasing the amount of contact time (7). Fontana and
lial cell lining will not happen and the epithelial cells will
colleagues used the three-time ethanol injection method.
continue secreting fluid cyst. In other words the cyst fluid
The amount of ethanol used in the treatment was up to
re-accumulates (4). Secretory epithelial lining the cyst
30% of the volume and did not exceed 60 ml per each cyst
wall must be destructed in order to prevent recurrence.
treatment. Free drainage method of the cyst was used. As
For this purpose, various sclerosing agents such as bis-
a result, recurrence of the cyst occurred in two patients
muth-phosphate (9), tetracyclin hydrochloride (10), ace-
and 68 cysts had complete resolution. The higher success
tic acid (11), povidone-iodine (12), n-butyl cyanoacrylate
rate in this study was based on the higher ethanol con-
and iodized oil (13), ethanolamine oleate (14), OK-432 (15)
centration at the cyst wall. The higher ethanol concentra-
and minocycline hydrochloride (16) have been used after
tion results in the greater destruction of the epithelial tis-
the cyst fluid aspiration. Ethanol is the most commonly
sue. Ethanol penetrates the fibrous capsule slowly that is
used sclerosing agent. Chemical properties of ethanol,
important in preventing systemic complication (19).
leading to necrosis of epithelial cells lining the cyst wall
There were limitations in this study. Four of the 88 cysts
will produce more obstacles. Secretory cells are rapidly
had treatment with 8F caliber catheter. The number of
inactivated by ethanol, but penetration of the fibrous
patients was not enough for the comparison. In other
capsule takes four to twelve hours. In this way, destruc-
words, there was not enough data to compare the choice-
tion of cysts occur without affecting the renal parenchy-
lock catheter and the 8F catheter. The second limitation
ma. Ethanol as a sclerosing agent has been mentioned in
was the pain scoring system. This is a retrospective study
the literature, and there are studies that have reported
and we did not have a scoring system for the treatment
success rates of over 90% (1, 2, 4). Akinci and colleagues
outcome related to pain. But now in our clinic we use the
treated 98 simple renal cysts with percutaneous ethanol
pain scoring system and check before and after the pro-
sclerotherapy with a single session technique (2).
At the end of the first year follow-up, the reduction rate in
In conclusion, percutaneous aspiration and ethanol
cyst volume was 93.1%. In 17 patients, the cyst disappeared
sclerotherapy is an effective way of treatment of simple
completely, and 83% of the patients had clinical improve-
cysts. Our study is the first paper that describes the usage
ment in the symptoms (2). Zerem et al. (17) treated 85 pa-
of trocar technique and choice-lock catheter.
tients and 92 cysts with percutaneous ethanol sclerother-
apy. Recurrence of only six cysts occurred at the 24-month
follow-up. Mohsen et al. (18) treated 64 cysts of 60 patients
There is no acknowledgement.
using sclerotherapy with 95% ethanol. In 84% the method
provided complete resolution. In our study, percutaneous
cyst aspiration and ethanol sclerotherapy of 88 cysts was
applied. Reduction in the size of the cyst occurred in all 75
Dr. Burak Ozkan, Dr. Baris Emiroglu, Dr. Ilker Arer and
patients and 88 cysts after the procedure. In 57 cysts, 80%
Dr. Ali Harman developed the idea and played great roles
reduction took place in the volume of the cyst after the
in the result and material section. Dr. Emiroglu and Dr.
procedure out of which 31 had a 60-80% decrease in size.
Aytekin carried out statistical analysis and wrote the dis-
Percutaneous ethanol sclerotherapy in the treatment of
symptomatic simple renal cysts were considered as suc-
cessful (P < 0.001). Our success rate was similar to other
studies. In the study conducted by Ozgur et al. (4), a num-
There is no financial disclosure.
ber of patients developed recurrence during follow-up
while a sclerosing agent was not used for any of them. In
our study, no recurrence or increase in the cyst volume was
reported during follow-up. We think that this is due to the
This study was not supported by any source from any
usage of ethanol as the sclerosing agent.
company or any grant from any hospital or such kind of
The single session of sclerotherapy with ethanol in the
institute. The funding organizations are public institu-
literature reported high success rates. There are also
tions and had no role in the design and conduct of the
studies indicating that multiple session sclerotherapy is
study; collection, management, and analysis of the data;
a more effective method of treatment. Hanna and Dahni-
or preparation, review, and approval of the manuscript.
ya have shown increased success rates after two sessions
of ethanol sclerotherapy. The recurrence rate was 80% in
the group on which only aspiration was carried out and
32% in the group on which percutaneous aspiration and
1. Bozkurt FB, Boyvat F, Tekin I, Aytekin C, Coskun M, Ozkardes H.
single-session ethanol therapy was performed. No recur-
Percutaneous sclerotherapy of a giant benign renal cyst with al-
rence occurred in the group on which ethanol sclero-
cohol. Eur J Radiol. 2001;40(1):64–7.
2. Akinci D, Akhan O, Ozmen M, Gumus B, Ozkan O, Karcaaltincaba
therapy was carried out twice. The high success rate of
M, et al. Long-term results of single-session percutaneous drain-
Iran J Radiol. 2014;11(2):e16327
Ozkan B et al.
age and ethanol sclerotherapy in simple renal cysts. Eur J Radiol.
12. Phelan M, Zajko A, Hrebinko RL. Preliminary results of percuta-
neous treatment of renal cysts with povidone-iodine sclerosis.
3. Hulbert JC, Hunter D, Young AT, Castaneda-Zuniga W. Percutane-
ous intrarenal marsupialization of a perirenal cystic collection-
13. Kim SH, Moon MW, Lee HJ, Sim JS, Kim SH, Ahn C. Renal cyst abla-
-endocystolysis. J Urol. 1988;139(5):1039–41.
tion with n-butyl cyanoacrylate and iodized oil in symptomatic
4. Ozgur S, Cetin S, Ilker Y. Percutaneous renal cyst aspiration and
patients with autosomal dominant polycystic kidney disease:
treatment with alcohol. Int Urol Nephrol. 1988;20(5):481–4.
preliminary report. Radiology. 2003;226(2):573–6.
5. Guazzoni G, Montorsi F, Bergamaschi F, Consonni P, Bellinzoni P,
14. Yamamoto K, Sakaguchi H, Anai H, Tanaka T, Morimoto K,
Centemero A, et al. Laparoscopic unroofing of simple renal cysts.
Kichikawa K, et al. Sclerotherapy for simple cysts with use of eth-
anolamine oleate: preliminary experience. Cardiovasc Intervent
6. Chung BH, Kim JH, Hong CH, Yang SC, Lee MS. Comparison of
single and multiple sessions of percutaneous sclerotherapy for
15. Ham WS, Lee JH, Kim WT, Yu HS, Choi YD. Comparison of multiple
simple renal cyst. BJU Int. 2000;85(6):626–7.
session 99% ethanol and single session OK-432 sclerotherapy for
7. Hanna RM, Dahniya MH. Aspiration and sclerotherapy of symp-
the treatment of simple renal cysts. J Urol. 2008;180(6):2552–6.
tomatic simple renal cysts: value of two injections of a sclerosing
16. Ohkawa M, Tokunaga S, Orito M, Shimamura M, Hirano S,
agent. AJR Am J Roentgenol. 1996;167(3):781–3.
Okasho A, et al. Percutaneous injection sclerotherapy with mi-
8. Israel GM, Bosniak MA. An update of the Bosniak renal cyst clas-
nocycline hydrochloride for simple renal cysts. Int Urol Nephrol.
sification system. Urology. 2005;66(3):484–8.
9. Holmberg G, Hietala SO. Treatment of simple renal cysts by per-
17. Zerem E, Imamovic G, Omerovic S. Symptomatic simple re-
cutaneous puncture and instillation of bismuth-phosphate.
nal cyst: comparison of continuous negative-pressure cath-
Scand J Urol Nephrol. 1989;23(3):207–12.
eter drainage and single-session alcohol sclerotherapy. AJR Am J
10. Kilinc M, Tufan O, Guven S, Odev K, Gurbuz R. Percutaneous in-
jection sclerotherapy with tetracycline hydrochloride in simple
18. Mohsen T, Gomha MA. Treatment of symptomatic simple renal
renal cysts. Int Urol Nephrol. 2008;40(3):609–13.
cysts by percutaneous aspiration and ethanol sclerotherapy. BJU
11. Kwon SH, Oh JH, Seo TS, Park HC. Efficacy of single-session per-
cutaneous drainage and 50% acetic Acid sclerotherapy for
19. Fontana D, Porpiglia F, Morra I, Destefanis P. Treatment of simple
treatment of simple renal cysts. Cardiovasc Intervent Radiol.
renal cysts by percutaneous drainage with three repeated alco-
hol injection. Urology. 1999;53(5):904–7.
Iran J Radiol. 2014;11(2):e16327
Source: http://iranjradiol.com/28708.pdf
Yonsei Med J 53(4):842-848, 2012 pISSN: 0513-5796, eISSN: 1976-2437 Fluoxetine Protects against Big Endothelin-1 Induced Anti-Apoptosis by Rescuing Kv1.5 Channels in Human Pulmonary Arterial Smooth Muscle Cel s FeiFeng Dai, ZhiFu Mao, Jun Xia, ShaoPing Zhu, and ZhiYong Wu Department of Cardiothoracic Surgery, Renmin Hospital of Wuhan University, Wuhan, China.
Center for Mental Health Policy Center for Mental Health PolicyVanderbilt Institute for Public Policy Studies Vanderbilt Institute for Public Policy StudiesVanderbilt University Vanderbilt University Tennessee's Adolescents in Publicly-Funded Treatment for Substance Abuse Problems: Baseline Interview Findings for TennCare Beneficiaries



