Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Evidencebasedmarketing.ca


Canadian Society of
Internal Medicine (CSIM)/Rocky Mountain
Conference Report - 24-27 November, 2011, Banff, Alberta
Dr. Robert Herman (Chair)
Dr. Michael Kenyon
Dr. Norm Campbell
Dr. Narmin Kassam
Dr. Jill Newstead-Angel
Rocky Mountain Conference Report Review Committee
Dr. Robert Herman
Dr. P. Timothy Pollak Dr. Kelly B. Zarnke
Dr. Gabriel Fabreau
Dr. Evan Minty
Professor of Medicine
Professor of Medicine
Head, Division of GIM
Internal Medicine Fellow
Internal Medicine Fellow
University of Calgary
University of Calgary
University of Calgary
University of Calgary
University of Calgary
Introduction to the 2011
offered to participants to learn from
KEYNOTE ADDRESS
Rocky Mountain /ACP
experts in specific topic areas; these well Top 5 Papers in General
General Internal Medicine attended workshops provided a valuable Internal Medicine 2010/2011
opportunity for collegial discussion and
Conference
Presented by Dr. Jake Onrot, University of British Columbia
Internists from Western Canada
As a value-added component and in
Every year, hundreds of papers related to
gathered in Banff, Alberta for the
an effort to enhance the educational
general internal medicine are published.
annual Rocky Mountain / ACP General
opportunities at the meeting, this
This makes staying up-to-date on the
Internal Medicine Conference held from
conference report provides a brief
latest evidence a formidable challenge for
November 24-27, 2011. This year's
summary of topics selected by
busy internists. Dr. Jake Onrot selected
conference continued its tradition of
the scientific committee. A clinical
five papers that were published in late
offering the more than 200 attendees
commentary follows each summary
2010 and in 2011 that he believes have
a stellar line-up of speakers from
to further reflect on and clarify how
had impact on the way internal medicine
academic and regional centres. Keynote
the findings might impact everyday
is practiced. Internists are encouraged
presentations and satellite symposia
clinical practice. Clinicians are
to read these papers and familiarize
covered a full array of state-of-the-art
encouraged to view and download
themselves with the context of each
topics in basic and applied research of
trial within the overall literature in its
the speaker presentations from
interest to general internists. Building
particular field, to balance the pros and
this year's conference at the Rocky
cons of each trial, and to apply the trial
on their popularity in previous years, a
Mountain Conference website at www.
evidence to their own decision-making.
series of small-group workshops were
Dr. Onrot introduced each of his selected
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
papers by first presenting it in the context fluid balance of 3L at 12 hours in
of apixaban to reduce the risk of
of a clinical case. The key findings and
sepsis patients; a more positive fluid
hemorrhagic stroke in patients with
conclusions from the five papers are
balance at 12 hours and at 4 days was
atrial fibrillation with a number-
summarized below:
associated with significantly increased
needed-to-treat (NNT) of 434 compared
1. The randomized controlled
to standard therapy with warfarin, and a
FEAST trial by Maitland et al. does
3. A randomized controlled trial by Garcia reduced risk of major bleeding (NNT 104).
not support the use of any fluid bolus
et al. supports the early use of
5. The POET COPD retrospective cohort
(albumin or saline) in critically ill
transjugular intrahepatic portosystemic study
supports the use of tiotropium
children with impaired perfusion in
shunt (TIPS) vs. traditional medical
versus salmeterol for the prevention
resource-limited African countries
therapy in patients with cirrhosis who
of exacerbations in patients with
because both significantly increased
were hospitalized for acute variceal
moderate-to-severe COPD.
48-hour mortality compared to
bleeding and at high risk for treatment
2. A retrospective review of the VASST
4. The large randomized controlled
trial by Boyd et al. supports a positive
ARISTOTLE trial supports the use
Maitland K, Kiguli S, Opoka RO, et al.; FEAST Trial Group. Mortality after fluid bolus in African children with severe infection. N Engl J Med 2011; 364(26): 2483-95. Epub 2011 May 26.
Boyd JH, Forbes J, Nakada TA, et al. Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med 2011; 39(2): 259-65.
Garcia-Pagan JC, Caca K, Bureau C, et al.; Early TIPS (Transjugular Intrahepatic Portosystemic Shunt) Cooperative Study Group. Early use of TIPS in patients with cirrhosis and variceal bleeding. N Engl J Med 2010; 362(25): 2370-9.
Granger CB, Alexander JH, McMurray JJ, et al.; ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011; 365(11): 981-92.
Vogelmeier C, Hederer B, Glaab T, et al.; POET-COPD Investigators. Tiotropium versus salmeterol for the prevention of exacerbations of COPD. N Engl J Med 2011; 364(12): 1093-1103.
Paper #1: FEAST trial
Paper #2: VASST retrospective review
illness severity. Patients with the lowest
For pediatric patients in resource-poor
The question of optimal fluid manage-
CVP had lower mortality. There was an
countries where malaria is prevalent,
ment in adults with septic shock was
interaction between survival, CVP, and
clinicians considering fluid manage-
assessed in a retrospective analysis of
fluid balance: patients with lower CVP
ment are faced with choosing between
VASST (VAsopressin in Septic Shock Trial). fared better with more fluid administra-
guidelines for first-world (i.e., 60 mL/kg
While the Surviving Sepsis campaign ad-
tion, whereas patients with higher CVP
isotonic solution) versus third-world (i.e., vocates for aggressive fluid resuscitation,
fared worse with more fluids. Optimal
reserve boluses for advanced shock) set-
recent literature reports that a more posi-
survival occurred in patients with a posi-
tings. FEAST randomized 3100 children tive fluid balance is associated with higher tive fluid balance of approximately 3L at with severe febrile illness and impaired
mortality. Dr. Onrot reminded the audi-
12 hours. The authors concluded that in
perfusion in sub-Saharan Africa to one
ence of the double-edged sword of fluid
"resuscitated" sepsis, the intravascular
of three fluid management strategies:
resuscitation: inadequate fluid administra-
fluid deficit and tissue hypoperfusion may
albumin bolus, saline bolus, or no bolus. tion may worsen tissue hypoperfusion
be corrected even though hypotension
The primary endpoint of the trial, 48-
and ischemia, whereas excessive fluids
and organ dysfunction may persist. In this
hour mortality, showed a benefit for no
may cause volume overload, pulmonary
setting, giving more fluid may be harmful.
bolus versus either bolus. Malaria (57%)
edema, capillary leak, and re-perfusion
The unaddressed question remains pre-
and anemia were prevalent. This result
injury. This prompted the retrospective
cisely when to stop administering fluids in
contrasts sharply with Rivers et al. (N
VASST data evaluation. Hypothesizing that septic shock.
Engl J Med 2001; 345: 1368-77), which
both too little fluid AND too much fluid
favoured early and aggressive fluid ad-
may be harmful, the analysis assessed the
ministration in adults with septic shock.
relationships between administered fluid
FEAST raises questions regarding routine volume, central venous pressure (CVP), administration of fluid boluses in other
and mortality. The results showed that
patient populations with shock.
a positive fluid balance predicts higher mortality, even after adjusting for baseline
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
more useful in assessing intravascular Further research is needed to volume than is a "normal" or elevated
improve our ability to reliably assess
These two studies highlight our
level and that fluid administration is
intravascular volume (e.g., stroke
limited knowledge regarding the
only one part of an early response
volume and pulse pressure variability
optimal level of fluid resuscitation
to sepsis that includes assessment
in response to fluid challenge,
and how we use imperfect indices
of other markers of tissue perfusion
bedside ultrasound [J Intensive Care
of tissue perfusion to make
(e.g., MAP, urine output, lactate,
Med 2009;24:329-37]) and tissue
iterative adjustments to our sepsis
cognitive performance, central
perfusion (e.g. lactate clearance and
management strategies. We are
venous pO2), early administration
measures of oxygen transport).
reminded that a low CVP or JVP is
of antibiotics and source control.
Paper #3: Early TIPS trial
Child-Pugh class C or B liver failure with
tially improved in the TIPS group com-
Acute and recurrent variceal bleeding is
persistent bleeding at the time of endo-
pared to standard therapy (ARR = 47%),
common in cirrhotic patients with portal
scopic band ligation (EBL) on vasoactive
as was mortality (ARR = 25%). Dr. Onrot
hypertension. The early use of TIPS has
drug therapy were randomized to TIPS
suggested that TIPS should be considered
not been considered a standard part of
within 72 hours or to standard therapy
in this patient population, arguing that
early management in preventing re-
(i.e., vasoactive therapy, beta-blockers,
we are often reluctant to adopt invasive in-
bleeding or death due to concerns about
then nitrates as tolerated and serial EBL
terventions that may turn out to be better
worsening hepatic encephalopathy. The
until variceal eradication). The primary
than medications.
study by Garcia-Pagan et al. suggests
endpoint of failure to control the acute
otherwise. In this study, 63 patients with
bleed or re-bleed at 1 year was substan-
were baseline differences between
Pugh B and C patients at high risk
treatment groups, including an
of rebleeding, early use of TIPS
Reservations have been expressed
asymmetry in encephalopathy.
should be considered along with
regarding the applicability of this
However, large benefits were
all standard effective and tolerated
trial, such as its small size; it is a
observed in clinically relevant
therapies (somatostatin analogues,
single trial showing benefit when
outcomes (rebleeding, mortality,
antibiotics, EBL, beta blockers and
a meta-analysis of related TIPS
hepatic function, and time in ICU
nitrates) while we await additional
research is more equivocal; the
and hospital) without adverse
subjects were highly screened and
effects on encephalopathy. Thus,
selected (<20% enrolled); and there
in appropriately selected Child-
Paper #4: ARISTOTLE trial
long-acting inhaled beta-agonists (LABA),
to severe exacerbation, and the number
To avoid redundancy, ARISTOTLE is sum-
based on patient preference, cost, and ad-
of moderate and severe COPD exacerba-
marized and discussed in another section verse effect profile, whereas patients with tions were all improved with tiotropium of this review.
more severe COPD (FEV1<50%) should be
compared to salmeterol. The effects were
treated with combination therapy. The
consistent across subgroups based on
Paper #5: POET COPD trial
question therefore remained, for patients
age, sex, COPD severity, smoking status,
The American Thoracic Society (ATS) rec-
with milder COPD, which monotherapy
body mass index, and use of concurrent
ommends that symptomatic patients with strategy is preferred? The POET COPD
inhaled glucocorticoids. Dr. Onrot con-
mild or moderate COPD (FEV1/FVC<70%;
study directly compared tiotropium to
cluded that for mild to moderate COPD
50%<FEV1<80%) should be offered bron-
salmeterol in more than 7000 patients
requiring monotherapy, a LAAC may be
chodilator monotherapy using either long- with COPD exacerbations and FEV1 <70% the preferred choice over a LABA.
acting inhaled anticholinergics (LAAC) or
for 1 year. The times to first exacerbation,
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
outcomes observed in POET COPD
enthusiastic and tenacious efforts
are statistically significant, some
to achieve smoking cessation in
The POET COPD illustrates the large
argue that the absolute size of the
patients who consume tobacco (like
trial size necessary to compare
differences (a few percentage points)
almost half of the POET COPD study
two active treatments using a
is not large. Even a trial of this size
population) will achieve a greater
meaningful outcome such as
is unable to definitively address
mortality benefit at a much lower
COPD exacerbations, such that the
questions of cardiac safety that
cost than any or all bronchodilator
similarity or small differences can
have been raised for both LABA and
therapies combined.
be determined with some degree of
anti-cholinergic bronchodilators.
certainty. While the differences in
Finally, we must never forget that
AM Edwards Lecture
topic of TB for nearly 30 years. He was
born. Over 100 years ago, William Osler
invited to present the 2011 AM Edwards said that TB is a social disease with
The Early Diagnosis of
Lecture, with the goal of sharing what
a medical aspect, and that remains
Pulmonary Tuberculosis
is important to know to identify TB
true in reserve communities today.
Dr. Richard Long, University of Alberta
early so that it can be appropriately
"Tuberculosis is a very sophisticated
Tuberculosis (TB) is frequently included
managed. Dr. Long challenged internists pathogen exploiting failures on our
as a differential diagnosis for respiratory to link seven key features that lead to a
part…. Each generation has failed
disorders, yet most internists do not
suspicion of TB.
to address social issues that are the
encounter the condition frequently
Tuberculosis in Canada is largely
basis of this disease," Dr. Long opined.
enough to be comfortable diagnosing
a disease that affects two groups:
Factors that converge when there is a TB
and managing patients with TB. Indeed,
aboriginals from Nunavut and to a lesser outbreak in a reserve community are: 1)
in Alberta only 110 to 180 cases of TB
extent on reserves across the Prairies and a delay in diagnosis of the source case,
are reported annually, meaning that
foreign-born people coming from high-
2) large numbers of susceptible contacts
internists may not see a case for many
incidence countries such as Asia and
(e.g., vulnerable children who have never
years. Dr. Richard Long, University of
Africa. This is important, given that 20%
been exposed to the infection), and
Alberta, has been an expert on the
of the Canadian population is foreign-
3) an environment that is favourable to transmission (e.g., malnutrition, overcrowding, poorly ventilated homes).
A combination of organ-specific as well as constitutional symptoms is the next clue for suspecting a case of TB. Dyspnea is uncommon in the early presentation of pulmonary TB because of its ability to interrupt both ventilation and perfusion in parallel. In an acutely infected patient, perfusion and ventilation is redistributed to the remaining healthy lung, leading to preserved function and ultimately, a delay in diagnosis. Typically, symptoms are subacute, occurring over weeks or months and sometimes years. The presence of any high-risk condition, including HIV/AIDS, organ transplantation, dialysis-dependent renal failure and patients on immunosuppressants, including systemic steroids, are another clue to diagnosing
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
TB, as these patients are at risk for
half, and assessing for the following
in tailoring treatment based on drug
primary infection and for reactivating
four common patterns: 1) upper lobe
susceptibility testing.
latent TB infection.
distribution, 2) cavitation, 3) volume
In Canadian-born patients, drug-resistant
Leukocytosis is typically a feature
loss, and 4) endobronchial lesions (fluffy, TB is rare thanks to the practice of
of community-acquired pneumonia,
poorly defined nodules are present in
directly observed therapy, which avoids
whereas anemia is a characteristic feature virtually all cases of TB). Finally, cases of
compliance issues. Drug resistance is
of chronic TB infection. Also, internists
suspected TB should be confirmed by
more commonly found in foreign-born
should not dismiss the value of a plain
sputum testing for definitive diagnosis,
infected individuals. Fluoroquinolones
CXR, which can provide several important with molecular epidemiology to link the
are bactericidal and can be lifesaving in
diagnostic clues. Dr. Long recommended infection to the source case spatially and
cases of highly drug-resistant TB.
dividing the lung into an upper and lower temporally. Recovery of the organism
through sputum samples is also helpful
through a call to the laboratory to
gamma release assays (IGRAs) for
ensure prompt diagnosis. In Alberta,
the diagnosis of latent tuberculosis
Despite medical advances, pulmonary all specimens collected are kept
(LTBI). These assays are in-vitro tests
tuberculosis remains an important
for culture of mycobacteria, which
of cell-mediated immune response
public health issue today. Dr.
although notoriously slow remains
measuring T cell release of interferon-
Long points out that TB has a
critically important as it allows for
gamma following stimulation by
disproportionate representation in
fingerprinting of the organism,
antigens specific to MTb. Until the
vulnerable populations in Canada,
susceptibility testing, and banking of
advent of these assays, the diagnosis
primarily aboriginal populations
individual strains.
of LTBI relied solely on the use of
and foreign-born immigrants. The
traditional tuberculin skin testing
importance of its early identification
In Dr. Long's second lecture, he
(TST), which has known limitations.
is compounded by its potential to
explained some of the recent
IGRAs have been shown to be highly
propagate within these communities
advances in testing for tuberculosis.
specific for LTBI, again 97%, but are
and the risk of TB in vulnerable
Two novel methods are becoming
not reliable in active TB infections
groups such as children and
widely available and must be
(sensitivity 75-90%) and unable
the immunocompromised (e.g.,
understood by internists. The first,
to distinguish between latent and
HIV/AIDS, patients with solid
known as nucleic acid amplification
active TB infections. Review of
organ transplant, and those on
testing (NAAT), is an automated
these assays by the Public Health
immunosuppressants). The recent
molecular test for Mycobacterium
Agency of Canada and Canadian
decision to withdraw the routine use
tuberculosis (MTb), which can be
Tuberculosis Committee released
BCG vaccine in Canada's First Nations
used for rapid diagnosis (within 2h
recommendations around their
and Inuit communities, which has
of collection) and to differentiate
use in 2008 (available at http://
been shown to reduce severe forms
MTb from other common forms
of TB such as CNS and disseminated
of mycobacterium such as
TB, makes children much more
Mycobacterium avian complex
php). Although IGRAs will likely
vulnerable to infection. This frames
(MAC). This test is highly sensitive
replace TST for the diagnosis of
the importance of early detection and
( 97%) and specific. Moreover, it has
LTBI, some important questions
prevention of local outbreaks.
also been shown to rapidly identify
remain. For example, their utility
drug resistant strains of TB through
in immunocompromised hosts
Once suspected, approaches focus
the use of line probe assays, which
and in healthcare worker screening
on early isolation, preferably airborne
is increasingly important as the
programs is unknown. Lastly, it is
isolation to prevent the spread of
incidence of multi-drug resistant
not known if a positive IGRA assay
TB. The gold standard for diagnosis
TB (MDR TB), both globally and
will remain positive for the life of the
remains recovery and culture of the
in Canada, continues to rise. This
patient, regardless of treatment for
organism. Microscopic detection
test was recently endorsed by
LTBI. Despite these questions, IGRAs
of AFB by stained sputum smears
the WHO and its utility shown in
represent a major advance in the
relates directly to the infectivity of
resource poor settings (N Engl J Med
diagnosis of latent TB.
a patient and, if clinical suspicion
2010;363:1005–15). The second
is high, these should be hastened
diagnostic test is the interferon
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Symposia
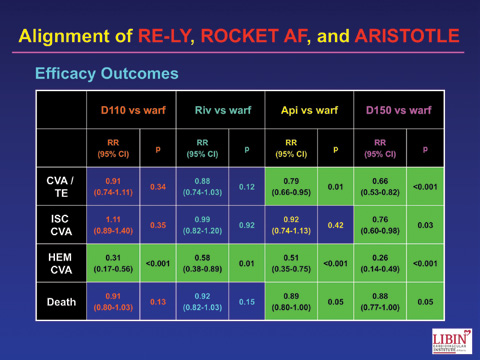
the risk of stroke in patients with
phase III trials evaluating dabigatran,
AFib by an impressive 64%. Aspirin
rivaroxaban, and apixaban versus
Evidence-Based Update in Atrial offers a smaller benefit that only
adjusted-dose warfarin. He noted that
Fibrillation: Review of Old and
reaches statistical significance with
each of these three trials was relatively
New Drugs for Anticoagulation the addition of other agents such as
large, enrolled patients with non-valvular
Presented by Dr. L. Brent Mitchell, Calgary clopidogrel. Even then, the benefit of the AFib and risk factors for stroke (i.e.,
Co-developed by the RM/ACP Annual
combination does not approach that of
patients who should be receiving an
Meeting Committee and Bayer Canada
warfarin. Based on these findings, the
anticoagulant), defined the primary
Anticoagulant therapy in patients with
CCS guidelines recommend that only
efficacy endpoint as stroke or systemic
atrial fibrillation (AFib) is a rapidly
patients at very low risk of stroke (i.e.,
embolism, and utilized major bleeding
evolving area of medicine. "New and
CHADS2 = 0) should receive aspirin; oral (with varying definitions) as a safety
emerging oral anticoagulants are
anticoagulant therapy is recommended
transformative and will change the
for all other patients.
The direct thrombin inhibitor dabigatran
way we practice." observed Dr. L. Brent
Warfarin's characteristics, including a
was evaluated in RE-LY.2 Compared to
Mitchell from the Libin Cardiovascular
narrow therapeutic window, substantial
warfarin, the 150 mg dose reduced the
Institute of Alberta as he opened his
heterogeneity in individual sensitivity,
risk of stroke with a similar risk of major
review of the evidence on this topic.
and multiple interactions with food,
bleeding and the 110 mg dose had a
Physicians have been aware of the
herbal agents, and other drugs,
similar rate of stroke with significantly
increased risk of thromboembolic
complicate its utilization in the clinical
reduced major bleeding. As a result of
events associated with AFib for over
setting. A recent meta-analysis1 found
these findings, the CCS guidelines now
100 years. Accounting for 15 to 20% of
that only 48% of patients with AFib were recommend that one of the new oral
all strokes, AFib is often undiagnosed
treated with warfarin, and of those,
anticoagulants such as dabigatran is
until after the stroke occurs. Strokes
the mean time in therapeutic range
preferred over warfarin in most patients
associated with AFib are more severe
was 55%. As Dr. Mitchell pointed out,
who require anticoagulation. The 150
than those occurring in patients without these findings tell us that only one
mg bid dose of dabigatran is generally
AFib. Importantly, the risk of stroke is
quarter of AFib patients are effectively
preferred over the 110 mg bid dose
equal for paroxysmal, persistent, and
anticoagulated, an important care gap
except in the elderly or patients with
permanent AFib.
that must be resolved.
reduced renal function. Warfarin may be preferred over dabigatran in patients
The 2010 Canadian Cardiovascular
Novel anticoagulants that address many at high risk of an acute coronary event.
Society (CCS) guidelines for
of warfarin's limitations are at varying
[Post-conference note: In 2012, CCS
thromboembolism prevention in AFib
stages of development. Dr. Mitchell
published a focused update to the
recommend all patients with AFib be
presented the key findings from the
guidelines that i) recommends one of
assessed for their risk of stroke, using a tool such as the CHADS2 score, and their risk of bleeding, using a tool such as the HAS-BLED score. In principle, patients with a HAS-BLED score of 3 or more are at an increased risk of major bleeding. However, many of the factors in the CHADS2 score are also included in the HAS-BLED score, making the practical interpretation of an elevated HAS-BLED challenging. Dr. Mitchell recommends that in situations where the HAS-BLED is elevated due to the presence of factors included in the CHADS2 score (i.e., hypertension, prior stroke, and age), then the risk of bleeding is secondary to the increased risk of stroke.
Warfarin has been the foundation for prolonged oral systemic anticoagulant therapy for many years and reduces
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
the new agents over warfarin in most
2 risk factors for stroke, a higher risk
were also slightly reduced bleeding
patients; and ii) removes the preference
population than was enrolled in RE-LY.
rates. Phase III results for edoxaban are
for warfarin over one of the new agents
Rivaroxaban was found to be non-
expected later this year.
in patients at high risk of an acute
inferior to warfarin for stroke prevention In considering the overall evidence
with similar rates of major bleeding.
from these studies, Dr. Mitchell
Three Factor Xa inhibitors are in the
Apixaban was compared to warfarin
emphasized that these new agents
late stages of development. [Post-
in the ARISTOTLE trial,4 which enrolled
are transformative and that healthcare
conference note: rivaroxaban received
patients at a similar risk for stroke as
providers will need to weigh the risks
a Notice of Compliance by Health
were studied in RE-LY. Apixaban reduced and benefits of each as they pertain
Canada for this indication in January,
the risk of stroke compared to warfarin,
to individual patients when making
2012.] The ROCKET-AF study3 evaluated although the ARR was only 0.34%,
treatment decisions.
rivaroxaban in patients with at least
which is not clinically meaningful. There
1. Baker WL, Cios DA, Sander SD, Coleman CI. Meta-Analysis to assess the quality of warfarin control in atrial fibrillation patients in the United States. J Manag Care Pharm 2009; 15:244-52.
2. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009; 361:1139-51.
3. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365:883-91.
4. Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981-92.
oral anticoagulant agents from which elderly (or to assume that a bleeding to choose, with widely available tests
event has the same disutility as a
Dr. Mitchell compared and
for therapeutic effect and agents
stroke), and in so doing, deny them
contrasted the three novel oral
for rapid reversal of their effects.
the benefits of stroke prevention.
anticoagulants that will likely
Healthcare providers involved in
This is especially important when
replace warfarin because of their
any aspect of thrombosis will need
one takes into account the fact
convenience and reliability. Although
to understand these agents and be
that by age 75, CHADS2 score
their absolute clinical benefit is
familiar with how to use them, and in increases to 1 by definition, at
similar to one another and each
what populations, in order to provide which point all patients without a
is comparable to warfarin, their
patients with best care. The relative
quantitatively high bleeding risk
reduced incidence of intracranial
advantages of each agent in any
should receive prophylaxis with
hemorrhage and practical
given patient population have yet to
systemic anticoagulation. Hopefully,
advantages are moving guideline
be worked out in real life practice.
the greater consistency of the newer
committees to recommend that
The adverse cardiac signal seen with
agents will lead to fewer bleeding
almost all patients with a CHADS2
dabigatran was not seen in the trials
complications and increased
score of 1 be fully anticoagulated
with the Xa inhibitors. Dabigatran
confidence in anticoagulating
rather than being considered for
and apixaban must be dosed twice
patients in this age group. This
aspirin prophylaxis.
daily, whereas rivaroxaban is given
new class of agents will change the
only once each day. All need to be
practice of medicine.
Dr. Mitchell correctly points out that
dose-adjusted in renal failure.
these novel oral anticoagulants are "game-changers." By the end of the
Finally, one must be careful not to
decade, there will be almost a dozen
overestimate bleeding risk in the
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Update on Diabetes:
The benefits and risks of intensive
Glycemic variability is another concept
Latest Evidence
glycemic control continue to be debated
that is generating interest in the
Presented by Dr. Stuart Ross, Calgary
in the scientific literature. The intensive
management of diabetes. Patients who
Co-developed by the RM/ACP Annual
glycemic control arm in the ACCORD
achieve "tighter" glucose control appear
Meeting Committee and Lilly/
study (target HbA1c <6%) was stopped
to achieve better outcomes than those
early due to a higher incidence of death
who experience more frequent swings
compared to standard management
from hyperglycemia to hypoglycemia.
In an era where clinical practice is
(target 7.0-7.9%). In contrast, the
In vitro studies have shown that cells
governed by evidence, it can be a
ADVANCE study reported a significant
exposed to greater variability in glucose
challenge to stay up-to-date on the
benefit of intensive glycemic control.
concentration have higher rates of cell
rapidly advancing field of diabetes
A sub-analysis of the ACCORD data
death than cells exposed to more stable
management. Dr. Stuart Ross, Clinical
showed that patients in the intensive
glucose concentrations. Studies have also
Professor of Medicine at the University of management group who died were
shown that glycemic variability predicts
Calgary, provided an update and a few
generally older, had a longer duration
mortality in adults in the ICU. A major
general conclusions on some of the most of disease, a longer interval between
trial called FLAT-SUGAR will prospectively
recent evidence in diabetes.
diagnosis and treatment initiation, a
evaluate the link between glycemic
The currently accepted glycemic target
history of cardiovascular disease, rapid
variability and cardiovascular outcomes
of HbA1c ≤7% was derived in large part
correction of elevated HbA1c, had
using continuous glucose monitoring.
from the UKPDS study, which showed
episodes of hypoglycemia, and continued Dr. Ross concluded his presentation
that this level of control was associated
poor glycemic control. In other words,
with a brief discussion of diabetic
with significant reductions in several
intensive management had failed in
nephropathy, which continues
diabetes-associated microvascular
these particular patients, even though
to be one of the most significant
complications. In a post-trial follow-
the mean HbA1c of the entire intensive
microvascular complications in diabetes
up of patients 10 years after the trial
control arm was 6.5%. These findings
patients. Renal impairment increases
was completed, patients who had
support the concept that optimal
the risk of hypoglycemia and some
been randomized to intensive control
management of diabetes depends on
oral hypoglycemic agents, such as
retained a significant advantage over
the "age and stage" of each patient.
metformin, are not recommended in
the conventional group, even if glycemic
Reaching a glycemic target of ≤7%
patients with impaired renal function.
control had deteriorated. This "legacy
in older patients with long-standing
However, evidence from a Cochrane
effect" suggests a major benefit of
diabetes and associated complications
review suggests the risk of lactic acidosis
early intensive glycemic management
may be more difficult – and potentially
associated with metformin is low and
for both microvascular and
harmful – compared to achieving this
this drug can be safely used in patients
macrovascular outcomes.
target in younger patients with less
with minor reductions in renal function.
advanced disease.
Sulfonylureas remain the recommended second-line therapy, but are also renally eliminated. Third-line treatment is insulin. DPP-4 and GLP are alternative 3rd line agents in patients who cannot take or refuse insulin. The DPP-4 inhibitors are excreted renally and dose adjustments are necessary in patients with impaired renal function (with the exception of linagliptin, which is excreted primarily through the bile). Finally, Dr. Ross advised that an appropriate glycemic target for an elderly patient with heart disease may not be <7%. "Common sense must remain a big part of clinical acumen."
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
potentially long lasting beneficial
4. High variability in blood glucose
effects in reducing complications
levels (glycemic variability) is
Diabetes continues to represent a
(the "Legacy Effect"). HbA1c targets
potentially harmful despite
very large burden of disease with
of <7% should ideally be achieved
achieving HbA1c targets <7%.
associated cost and morbidity in
within one year of diagnosis of
Canada. Review of Canadian data in
5. The therapeutic pyramid should
diabetes care reveals discouraging
include metformin as the first line
results with respect to achieving
2. Simultaneous management of all
agent, sulfonylureas as second
combined targets of glycemic control, cardiovascular risk factors,
line, and insulin as third line.
blood pressure and lipid control
including hypertension and
Insulin is a more effective therapy
(Can J Cardiol 2010;26(6):297–302).
dyslipidemia, is paramount.
than oral agents and internists
Dr. Ross' review offered five very
need to be more willing to initiate
practical and evidence-based
3. Elderly patients with a long history
this therapy in hopes of achieving
recommendations for internists to
of diabetes and difficulty achieving
glycemic targets earlier in the
manage their diabetic patients:
glycemic targets may be harmed
disease process.
by overly aggressive management
1. Early management in newly
of blood sugar control.
diagnosed patients offers
Update on Lipids:
on biomarkers and new evidence linking
mediators have a major role in the
Cardiovascular Disease
atherosclerosis with inflammation.
pathophysiology of atherosclerosis,
Prevention - A Look Ahead
Studies suggest that for each 1 mmol/L
and patients with chronic inflammatory
Presented by Dr. Jacques Genest,
reduction in LDL-C there is a 2% absolute
disorders such as rheumatoid arthritis
McGill University
risk reduction in major atherosclerotic
and psoriatic arthritis have a 2- to 5-fold
Co-developed by the RM/ACP Annual
events, regardless of the lipid-lowering
higher incidence of cardiovascular
Meeting Committee and Merck Canada
agent employed. Whereas evidence
disease. Emerging evidence suggests that cholesterol crystallization may
Canadian guidelines for the diagnosis and continues to accumulate supporting the
be an early inflammatory trigger of
treatment of dyslipidemia and prevention
benefits of aggressive LDL-C lowering,
atherosclerosis. Current models propose
of cardiovascular disease are updated
strategies involving modulation of HDL-C
that cholesterol crystals activate the
every 3 years. It is expected that the 2012 mass and function have not borne
inflammasome to generate interleukin
version of the guidelines will be largely
consistently positive results. The results
unchanged in terms of cardiovascular risk
of ongoing studies evaluating the effects
β, triggering production of CRP
by the liver and ultimately resulting in
assessment and LDL-cholesterol (LDL-C)
of niacin, dalcetrapib, and anecetrapib on
vascular inflammation. The potential
treatment targets. Dr. Jacques Genest,
cardiovascular event are eagerly awaited.
involvement of the inflammasome and
McGill University, reviewed some of the
Dr. Genest predicted that vascular
ongoing studies that may influence future
β pathway opens the door to new
inflammation may play an increasing role
molecular targets for the treatment of
guideline recommendations with a focus
in atherosclerosis research. Inflammatory
atherosclerosis.
function may be more important than
written, HPS-2 THRIVE and AIM-HIGH
its mass. This was a hard learned
(N Eng J Med 2011;365:2255–67)
Dr. Genest's talk is an excellent
lesson in ILLUMINATE (torcetrapib) (N
give credence to the current focus
resource to general internists as
Eng J Med 2007;357:2109–22), and
on getting LDL to target. The first
they navigate this dynamic field.
one that has informed forthcoming
advice to pass on to our patients: Eat
The signal in JUPITER (Circulation
studies of the next generation
food. Mostly plants. Not too much
2010;121:143:50) regarding hs-CRP
of CTEP inhibitors, namely DAL
(Pollan M. The Omnivore's Dilemma:
indicate that the protein itself is not
OUTCOMES (dalcetrapib) and REVEAL
A Natural History of Four Meals. New
likely a causal factor in coronary
(anacetrapib). Although the next
York, New York: Penguin, 1996).
artery disease. Modulation of HDL
chapter for niacin remains to be
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
CRT in the Treatment of
in the primary composite endpoint of
but there was no significant benefit of CRT
Heart Failure
total mortality or heart failure events
added to ICD in this subgroup of patients.
Presented by Dr. Anthony Tang, Victoria,
was demonstrated in Class I-II patients
However, there was a trend towards a
and Dr. Jonathan Howlett, Calgary
receiving CRT plus an implantable cardiac
reduction in hospitalization due to heart
Co-developed by the RM/ACP Annual
defibrillator (ICD) compared to ICD alone
failure (hazard ratio 0.58, p=0.052). A
Meeting Committee and Medtronic
in the MADIT-CRT study; however, the
small Italian study suggests that CRT can
difference was driven by the reduction in
be effectively applied in patients with
While clinical trial evidence supporting
heart failure events, with no significant
AF who undergo AV junction ablation. A
cardiac resynchronization therapy (CRT)
difference in mortality. Both studies
subsidiary study is now being planned to
initially accumulated for the treatment
reported a significant reduction in left
address this particular group of patients.
of Class III and IV heart failure patients,
ventricular (LV) volume and increased
recent studies have shown benefits in
Dr. Jonathan Howlett, Clinical Professor
ejection fraction (EF) from baseline – so
mildly symptomatic patients. Indeed,
of Medicine at the University of Calgary,
called ‘reverse remodeling' of ventricular
the REVERSE, MADIT-CRT and RAFT
used a case-based approach to review the
studies support a reduction in morbidity,
recently updated Canadian Cardiovascular
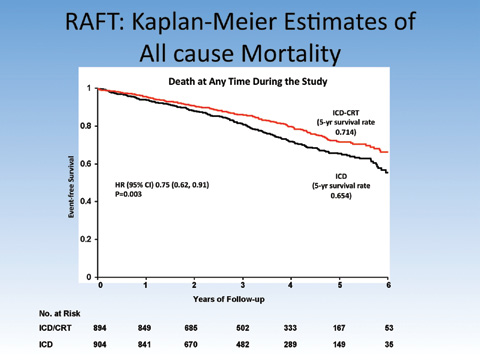
mortality, and disease progression in Class The RAFT trial, which was largely a
Society (CCS) heart failure guidelines
I or II heart failure patients. Dr. Anthony
Canadian study, supports a significant
with a focus on CRT. The guidelines
Tang, Professor of Medicine at the
reduction in a composite endpoint of
strongly recommend the use of CRT in
University of British Columbia, reviewed
mortality or hospitalization due to heart
combination with an ICD for heart failure
the clinical trial evidence for CRT in the
failure in Class II-III patients receiving
patients on optimal medical therapy with
management of patients with mild-to-
ICD plus CRT. The RAFT trial showed a
Class II symptoms, LEVF <30% and QRS
moderate heart failure.
significant benefit in terms of all-cause
duration of 150 ms.
mortality, with an absolute reduction
The REVERSE study demonstrated a trend
Dr. Howlett pointed out several patient
of 6% over 5 years of follow-up. A
toward less worsening of a composite
features that should be considered
prespecified subgroup analysis showed
endpoint that included all-cause mortality,
when selecting patients for CRT referral,
that patients with a wider QRS duration
heart failure hospitalization and heart
including the severity of heart failure (i.e.,
or left bundle branch block (LBBB) derived
failure worsening in Class I-II heart failure
ejection fraction, symptoms, rhythm,
greater benefit from the addition of CRT.
patients receiving CRT compared to those
QRS width and morphology, likelihood of
with an implanted but inactive device (16% Patients with permanent atrial fibrillation
successful pacing) as well as comorbidities
vs. 21%, p=0.10). A significant reduction
(AF) were also included in the RAFT study
and patient preference. Internists should keep in mind that studies to date have not included patients with planned surgical or interventional procedures, recent myocardial infarction, known cardiomyopathies, end stage renal failure, dementia, or other significant life-limiting co-morbidities. Therefore the benefits and risks of CRT in these patients remain unknown. In conclusion, Dr. Howlett summarized some of the points that argue for and against CRT.
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Features that argue for CRT
Features that argue against CRT
Lower ejection fraction
Ejection fraction closer to 35%
Lack of sinus rhythm, lack of pacing potential (e.g., large posterior infarct)
QRS closer to 150 ms
QRS closer to 120 ms
Stable, chronic heart failure
Extremes of symptoms
• Use of inotropes
• Female gender?
• Acutely worsening or intermittent symptoms
there was a 3.7 % absolute reduction
EF < 30% and a QRS duration > 150
in mortality. These numbers are quite
msec be considered for placement of
A recently published systematic
respectable. However, because of the
CRT-ICD clearly have not examined
review and meta-analysis on the
high mortality and morbidity in this
all of the economic issues relevant
subject of CRT (J Cardiac Fail
cohort, 3-6 times more people died
to implementing such a costly new
2011;17:860-6) cites 5 studies
or were admitted to hospital for heart
technology in this sizable population
that compare CRT to medical
failure despite having the device than
of patients. Will there be more money
management of heart failure alone
benefited from it.
for this exciting new technology,
in patients with Class II - IV heart
or is the verdict in from the 3 trials
failure. Summarily, these studies
The authors of the 2011 CCS
presented and it's Code BLUE on
show a 4.5% absolute reduction in
Heart Failure Guidelines statement
CRT? Perhaps there is a subset of
mortality over the 1-2 years of the
suggesting that all patients with
patients with heart failure where CRT
running of the trials. Also, in 6 RCTs
NYHA Class II-IV heart failure despite
or some better treatment will help
comparing CRT-ICD versus ICD alone
optimal medical treatment with an
them live longer, healthier lives.
Short Snappers
(those with previous stroke, or pre-
example, the recent HYVET-COG study
existing cognitive impairment). While
showed that aggressive blood pressure
Dementia: A Disease of the
this association would be expected for
reduction (i.e., -15 mmHg) in very elderly
vascular dementia, it also applied to
patients significantly reduced their risk
Presented by Dr. Tom Jeerakathil,
patients with Alzheimer's disease (AD).
of dementia. The curves continued
University of Alberta
The findings are also consistent with
to diverge over time, suggesting that
Stroke and other vascular risk factors
the 1997 Nun Study, which showed
dementia might be delayed or prevented
are associated with an increased risk
that in the presence of microinfarcts,
by controlling blood pressure over
of future dementia. How this occurs
smaller plaque burden produced more
several decades.
and the extent to which cardiovascular
significant cognitive impairment. Other
While more definitive evidence linking
risk factors and small vessel disease
cardiovascular risk factors have also been dementia with small vessel disease
contribute to dementia is less well
associated with a higher risk of dementia continues to emerge, Dr. Jeerakathil
established. The findings of a recent
and cognitive changes, particularly
suggested that internists should consider
meta-analysis of prospective longitudinal hypertension.
adopting quick screens for cognition into
studies that examined the impact of
If dementia is a disease of the
routine practice. The Mini-Cog test (Int J
white matter changes on outcomes
microcirculation, can controlling
Geriatr Psychiatry 2000;15:1021–7) was
including cognitive decline, dementia,
cardiovascular risk factors modulate
highlighted as a screen that takes 2 to 4
stroke and mortality support an
disease outcomes? The literature
minutes to administer and correlates well
association between small vessel disease shows mixed results, but there is a
with MMSE and MoCA scores.
and dementia in the general population,
signal suggesting that modulation
although not in ‘high risk' subgroups
of risk factors may be protective. For
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
and in gross pathology between
to consider increasing their use of
vascular dementia and AD may, in
neurocognitive screening tools given
Dr. Jeerakathil's talk raises the
fact, reflect a common etiological
the prevalence of vascular risk factors
interesting hypothesis that the
origin with respect to microvascular
within our patient population.
overlap that is seen both clinically
health. General internists may want
Use of Hypertonic Saline in
Therefore, guidelines suggest empiric
acceptable. Reasonable limits for the
treatment with hypertonic saline. There
treatment of acute severe hyponatremia
Presented by Dr. Irene Ma,
are at least four formulae available to
are to increase sodium by 1-2 mEq/L/hr
University of Calgary
guide the amount of hypertonic saline to for the first 3-4 hours, never exceeding administer, with the Androgue-Madias
3/hr, with a daily maximum of 8-12
The treatment of hyponatremia involves
formula being the most commonly used. mEq/L.
balancing the risks of cerebral edema
While the equation seems deceptively
from undertreatment and the risks of
While there is clearly potential harm
simple, it can be difficult to recall when
osmotic demyelination syndrome (ODS)
to correcting an acute drop in sodium
a patient is actively seizing and requires
with over-aggressive treatment. Evidence
too rapidly, correcting sodium levels
immediate care. Dr. Ma recommended
guiding the optimal management of
too slowly can also result in negative
a simpler method that yields the same
hyponatremia is limited and is based
outcomes. In acute hyponatremia, a
answer as using a formula, but that does
primarily on consensus from expert
correction rate of 2 mmol/hr has been
not require any memorization on the
panels. Nonetheless, when confronted
associated with greater survival than
internist's part. The method involves
with a patient with symptomatic severe
correcting sodium more slowly. Studies
logically working through the following
hyponatremia, few internists would argue
suggest that end sodium values are
against the use of hypertonic saline.
overestimated about 75% of the time
1. How much sodium is in the patient
using the available formulae. Dr. Ma
Hypertonic saline is any solution with
right now? [TBW (L) x existing serum
argued that clinicians should no longer
a higher sodium concentration than
sodium concentration (mEq/L)]
be surprised when patients are over-
the body's normal level of 140 mEq/L.
corrected, but rather, they should expect
Typically, hypertonic saline solutions are
2. How much sodium will be in the
this to be the case. There are multiple
3% (513 mEq/L) and 5% (856 mEq/L), but patient if 1L of 3% hypertonic saline is
reasons that may account for over-
they can range as high as 29%. The use
administered? [#1 above + 513 mEq]
correction using formulae. For example,
of hypertonic saline is generally guided
3. What would the patient's end sodium
formulae do not account for ongoing
by symptoms. Patients who are most
concentration be? [#1 above + 513]
urine and gastrointestinal sodium losses,
likely to do poorly if undertreated include mEq / [TBW + 1] L
dietary intake, and more importantly,
those with an acute drop in their sodium, 4. How quickly do you want to achieve
for water diuresis. This makes ongoing
women, children, and patients who are
this end concentration?
laboratory testing and monitoring
essential in the management of acute
In order to avoid overtreatment of
Hyponatremia can be worsened if the
hyponatremia. When sodium is over-
hyponatremia and the risk of OSD,
saline solution administered does not
corrected, hypotonic solutions can be
there are recommended limits based
have a higher sodium concentration
administered (e.g., 1-2 μg IV/SC DDAVP)
on human data from different sources.
than that in the urine. However, when
with monitoring of urine sodium levels
While these vary, Dr. Ma suggested
internists are confronted with an acute
every 1-2 hours to ensure they remain in
that for undifferentiated symptomatic
case of severe hyponatremia, urine
the normal range.
hyponatremia, <12 mEq/L/day is
indices are not always readily available.
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
the response to your sodium
with 0.9% saline. First, and this
was discussed by Dr. Ma, if the
Is there any risk to giving 100 ml of
tonicity (osmolality) of the urine
3% NaCl (or 2 ml/kg in smaller adults
What about using normal (0.9%)
is higher than the tonicity of the
or children) over 5-10 min, repeating
saline for correction of hyponatremia? solution you are using to correct
the serum sodium and thereby
If you know the concentration of
the hyponatremia, rehydrating/
devising an ‘on-the-go' replacement
solute in a bag and can correctly
correcting with 0.9% saline may drive
strategy? This can be continued until
calculate the amount and the rate
the sodium lower and worsen the
the patient is asymptomatic (usually
at which you wish to administer it
hyponatremia. Second, given that
after a correction in serum sodium
(information needed regardless of the 0.9% saline has inherently more water
by 4-6 mEq/l), following which no
solution you are choosing), the only
than 3% saline, you risk correcting
further sodium correction or a slower
difference in giving 100 mEq of Na+
the volume deficit before correcting
rate of sodium administration can
as 0.9% NaCl or 100 mEq of Na+ as
the sodium deficit. The stimulus
be undertaken depending upon the
3% NaCl is in the amount of water you causing ADH secretion is lost (ADH is
cause of the hyponatremia (Curr
are providing along with that solute.
appropriately elevated in hypovolemic
Opin Crit Care 2011;17:581-93).
The clinical question becomes ‘How
hyponatremia) in which case the
In no instance should the daily
much water would I like to give to this kidney starts excreting large volumes
correction be greater than 10 mEq/l
patient who is already hyponatremic?'
of dilute urine thereby self-correcting
in the first 24 hours and 18 mEq/l
This, of course, relates to the
the hyponatremia, irrespective of
over 48 hours. Indeed, given the
overriding cause of the hyponatremia
your best efforts to control solute and
frailties of assessing volume, most
and to the risks inherent in
water administration. Incidentally, the
experts now suggest giving repeated
same problem awaits glucocorticoid
small boluses of hypertonic saline
If the patient has hypovolemic
administration in hyponatremia
and repeatedly measuring serum
hyponatremia, and so is deplete
due to adrenal insufficiency. Thus,
sodium to all symptomatic patients
of both sodium and water but
hypertonic saline should be the
that require sodium correction (Acta
proportionally more sodium than
principal replacement solution early
Anaesthesiol Scand 2011; 55:139-
water, 2 conditions may complicate
in the treatment of most cases of
48). The key is, and this cannot
your correction, particularly when
hyponatremia, irrespective of the
be overemphasized, choosing the
choosing to rehydrate/correct
correct solution and reassessing
Exercise in health promotion
osteoporosis, diabetes, coronary heart
Current exercise recommendations call
Presented by Dr. Mark Roberts,
disease, colorectal cancer, breast cancer, for at least 30 minutes of moderately
University of British Columbia
hypertension, and many others. Given
intense physical activity at least 5 days
the health benefits of physical fitness
per week, and preferably every day. These
Current epidemiological reports suggest
and exercise, it might be expected that
recommendations are based on evidence
that low fitness levels are responsible for healthcare professionals would routinely suggesting that the benefits of exercise
more deaths in Canada and the USA than advise their patients on this important
extend beyond weight control and weight
chronic diseases such as hypertension,
matter. Yet studies suggest this is not
loss. Physicians should therefore be
obesity and smoking that are expensive
the case. Indeed, in a study of 330 family actively recommending the minimum
to treat and garner much more attention. physicians across Canada, only 11%
amount of exercise to all of their patients.
In Canada, it is estimated that 30,000
counselled their patients on the benefits
While higher amounts of exercise may be
deaths can be attributed to the "sedentary of exercise, and more alarmingly, only
necessary in some circumstances, such as
death syndrome." Low fitness is not only
43% felt they should be counselling their
endurance training, there are undeniable
an important risk factor for mortality, it
patients on this topic. Not surprisingly,
health benefits from meeting just the
is also associated with a host of other
the major barriers against counselling
minimum requirements for physical
chronic conditions including dementia,
were time and education about exercise.
activity each day.
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Roberts' talk, the American College of scenario, where limiting our daily Preventative Medicine has noted that
sitting / laying to 23.5 hours proves
Dr. Roberts presented discouraging
the health benefits of regular physical
too ambitious, a recent analysis of
statistics regarding physician
activity extend beyond weight loss.
the INTERHART study offers some
advocacy for exercise despite the
General Internists may want to avail
hope that even mild to moderate
existing evidence about its benefits,
themselves of this fact to help keep
occupational activity is protective (Eur
and the cost effectiveness of physical
patients motivated in the absence of
Heart J 2012;33:452–66). See you all
activity interventions (Br J Gen Pract
a demonstrative change in physical
in the stairwell.
2011;61:e125-33). As cited in Dr.
appearance. In the worst case
Workshops
can all be well visualized with bedside
Dr. McDermid utilizes U/S-guided
U/S. Studies suggest that non-cardiology bedside diagnosis 3 to 4 times during a
Ultrasound Guided Bedside
intensivists can reliably perform goal-
typical night on call. "My practice revolves
Diagnosis & Procedures
directed U/S. For example, a study of
around U/S because I can get information
Presented by Dr. Rob McDermid,
six intensivists who received ten 1-hour
fast. It helps me improve the care of my
University of Alberta
sessions of U/S training were found to
patients." Guidelines are currently in
Ultrasound (U/S) technology has the
perform with 84% accuracy. Moreover,
development for the training and optimal
potential to assist physicians with a host
the information obtained by bedside U/S use of bedside U/S. Meanwhile, the
of procedures and diagnostics, including resulted in a change in management
availability and portability of U/S devices
central venous access, thoracentesis,
strategy in 37% of cases. Trainees at all
is increasing while the development of
and many others. Bedside U/S has
levels can learn how to apply bedside
accurate and affordable U/S probes is
been shown to be particularly useful
U/S-guided diagnosis with appropriate
an ongoing area of innovation. A hand-
for identifying cardiac abnormalities
training. For example, first-year medical
held U/S device is now available for
(low ejection fraction, high pulmonary
students have been taught to use
pressure, pericardial effusion, and severe bedside U/S to augment diagnosis. valvular regurgitation or stenosis). These
are safer when guided by U/S. But,
practices. Training programs with
how extensively should internists
established curricula (both U/S theory
Will bedside US become the new
not formally trained in diagnostic
and learning of specific skills) exist.
stethoscope of the 21st century?
imaging be using this modality of
However, the occasion would be rare
This technology has great potential
investigation? While very limited
that a bedside U/S replaces formal
to augment our physical exam skills
research in this area is supportive of
and complete diagnostic imaging,
and to enhance the safety of some
the capacity for health care providers
when indicated. This technology
of our common bedside procedures.
at many levels to learn very specific
is undoubtedly useful for many
For example, physical exam findings
U/S skills, there is much to learn
applications and is evolving rapidly
such as thyroid enlargement or
regarding optimal introduction of
– for example, the hand held-device
nodules or the presence of a pleural
this new technology into practice.
cited above. As internists, it behooves
effusion or ascites can be confirmed
ED physicians and intensivists
us to keep up to date not only in our
at the bedside. Central venous
have moved ahead of internists on
knowledge base but also evolving
catheterization and thoracocentisis
introduction of bedside U/S into their
diagnostic skills.
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Infection in Pregnancy
no associated medical conditions. The
Finally, Dr. Castillo advocated for the
pathogens most often associated with
recognition of pregnancy as a window
Presented by Dr. Eliana Castillo, University of Calgary
maternal sepsis leading to mortality
of opportunity to promote routine
include Group A Streptococcus, E. coli,
vaccination. Immunization against
Pregnancy can be considered as a
and influenza. Furthermore, almost
influenza can significantly reduce
"controlled" or contained form of
50% of women who died did so within
maternal morbidity and mortality, and
systemic inflammatory response
24 hours of admission, supporting the
it can also protect newborns from
syndrome (SIRS) whereby heart rate
concept of rapid deterioration when
death in the early days of life. Mothers
is >90 bpm, respiratory rate is >20
decompensation occurs. These data
expressing concerns regarding the
breaths/min, PaCO2 is <32 mmHg,
suggest a failure of taking routine
theoretical risks of vaccination during
white blood cell count is >12,000, and
observation, asking for specialist advice
pregnancy can be reassured that the risk
temperature is higher than 38˚C or less
early, and importantly, starting empiric
of adverse pregnancy outcomes due to
than 36˚C. These are normal physiologic antibiotic treatment in pregnant women vaccine-preventable infections is much
changes in pregnancy and women often
when sepsis is suspected. Dr. Castillo's
higher. The World Health Organization
feel fine despite their presence.
own data involving 75 cases of sepsis
recommends routine vaccinations
Infections are common complications
among pregnant women admitted to
during pregnancy including influenza
of pregnancy, occurring in 1 to 10%
the British Columbia Women's Hospital
and DTap, as well as specific vaccines
of pregnant women. In the setting of
suggest that SpO2 was measured in only
based on maternal comorbid medical
contained SIRS, a pregnant woman can
42% of cases, urine output was recorded
conditions. Despite this recommendation
usually compensate for an infection for
only 20% of the time, and lactate was
and the recognized risks of influenza
a while. However, if she decompensates,
ordered <1% of the time.
infection during pregnancy, only 15%
it tends to happen rapidly. Sepsis is
Recommendations include considering
of all pregnant women are immunized,
often not recognized soon enough
tachypnea and/or an SpO
suggesting an educational need for
in pregnant patients because the
than 94% on room air to be red flags,
patients and physicians alike.
physiology of pregnancy can mimic
ensuring that perfusion goals (urine
the pathophysiology of sepsis. Sepsis
output, lactate) are met, directing
continues to rank among the top three
investigations toward identifying a source
causes of maternal morbidity in the
(nasopharyngeal swabs and sputum), and
United Kingdom and Canada, where
tailoring appropriate antibiotic treatment.
data on maternal deaths are tracked
With the exception of fluoroquinolones,
and compiled every 3 years. This rich
any antibiotic that would typically be
source of epidemiologic information
used for the treatment of respiratory
suggests that the median age of women
infections in non-pregnant patients (e.g.,
who die from sepsis during pregnancy
macrobid, azithromycin, 3rd generation
is 34 years, and about half of these
cephalosprins) can be considered for
women were otherwise "healthy" with
pregnant women.
Dr. Castillo gave an informative and insightful presentation on this subject and we would encourage participants to review her slide set on the RM website.
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Osteoporosis for General
life) and the healthcare system (i.e.,
loss or family history of hip fracture,
Internists
about $1 billion per year in Canada).
which increases the absolute 10-year
Presented by Dr. Bill Leslie,
The new guidelines endorse the use of
risk by 9%. Spinal imaging can be
University of Manitoba
the CAROC risk assessment tool that
useful in moderate-risk patients; if any undiagnosed vertebral fractures are
The Osteoporosis Canada clinical
is based on national fracture mortality
identified, the patient is re-categorized
practice guidelines for the diagnosis
data and has been tested and validated
into a high-risk group that warrants
and management of osteoporosis were
in Canadian cohorts. This simple tool
treatment. There is strong evidence to
updated in 2010. Although they continue emphasizes just three risk categories
support osteoporosis treatment in high-
to emphasize T-scores and bone mineral (low, moderate and high) and three risk
risk patients (10-year risk >20%). There
density (BMD) for the characterization
factors (age, sex and BMD), which are
are several first-line therapies available
of osteoporosis, the new guidelines also
generally sufficient to inform appropriate to choose from. Dr. Leslie noted that
recognize that this disease is complex
treatment decisions. Alternatively, Dr.
while serious adverse events such as
and multifactorial, and that more than
Leslie suggested using the World Health
osteonecrosis of the jaw and atypical
one single risk factor predicts fracture
Organization's FRAX system, which
femur fractures have been associated
risk. Therefore, the new guidelines have
considers additional risk factors. A
with bisphosphonate therapy, these
increased their focus on fractures and the Canadian version is available, which has
events are very rare and the risk-benefit
clinical impact of fragility fractures.
been directly validated in a Canadian population. Both tools estimate 10-
ratio remains favourable in high-risk
There continues to be an enormous care
year fracture risk, which aligns with
patients. New anabolic treatments
gap in post-fracture care and treatment
the Osteoporosis Canada treatment
that regulate osteoclast function are in
of high-risk patients to prevent secondary guidelines, and are available on the
development and Dr. Leslie predicted
fractures. This is in stark contrast to
Osteoporosis Canada website (www.
that "these new drugs will change how
other chronic health conditions. For
osteoporosis.ca).
we treat osteoporosis in the next 5 to
example, 80% of patients who suffer
a heart attack are discharged from
Patients with a low 10-year risk of
Calcium and vitamin D supplementation
hospital with a prescription for beta-
fracture (<10%) are unlikely to benefit
as well as weight-bearing exercise
blockers, whereas only 15% of people
from treatment; lifestyle counselling
remain important components of
who fracture are diagnosed and treated
should be dispensed and the patient
management for patients with low
for osteoporosis. The consequences of
reassessed in 5 years. Patient preference
bone mass. Current recommendations
under-recognition of osteoporosis can
guides treatment decisions for the
suggest an upper limit of 1200 mg/d of
be considerable to both patients (e.g.,
moderate risk (10-20%) group. These
calcium from both dietary sources and
subsequent fracture, hospitalization,
patients should be evaluated for
supplements, a reduction from previous
institutionalization, reduced quality of
additional risk factors, including height
recommendations of 1500 mg/d. Some studies have suggested that calcium supplements may cause a surge in serum calcium levels that can increase the risk of cardiovascular disease. However, Dr. Leslie cautioned that the evidence for this association is limited to one large study that found a signal using a very narrow definition of myocardial infarction, but the association disappeared when adjudicated definitions were used. Dr. Leslie is comfortable recommending 1200 mg/d, whereas there is no evidence for benefit above this level. He advises vitamin D supplementation at 1000-2000 IU/d, although guideline recommendations vary between 800-4000 IU/d.
A Quick Reference Guide for the 2010 Osteoporosis Canada guidelines is available online at www.osteoporosis.ca.
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
formal assessment of osteoporosis
active life style that includes weight-
risk in all patients with fractures as a
bearing exercise and to consider an
Efforts to reduce the clinical and
first step to avoiding repeat breaks.
intake of 1000-2000 IU/d of Vitamin
financial costs of osteoporosis
Both the CAROC risk assessment tool
D as well as a total food/supplement
continue to be frustrated by the
and the World Health Organization's
intake of 1200 mg/d of calcium.
inability of any single intervention
FRAX system provide a 10-year
By the time the bone becomes
to have a major impact on this
fracture risk, validated for the
osteoporotic enough to fracture,
multi-factorial problem. However, a
Canadian population. Those with a >
it may be too late to fully regain
systematic approach to diagnosis,
20% risk merit strong consideration
its integrity. Therefore, as in many
categorization and treatment will still
for bisphosphonate therapy.
medical diseases, prevention is far
be needed for there to be any hope of
more desirable than cure.
improving the situation.
Dr. Leslie's workshop also reminds us that the most prudent therapy is
The new Osteoporosis Canada
preventive. Younger patients need
guidelines start by recommending
encouragement to participate in an
Update on Perioperative
event surveillance, and dispensing
(American Society of Anesthesiologists)
Medicine
general medical advice. Dr. Bruce Fisher
physical status classification system,
Presented by Dr. Bruce Fisher,
reviewed the benefits – and potential
Lee criteria, and the revised Cardiac Risk
University of Alberta
harms – of performing preoperative
Index (rCRI) are the most commonly
cardiac risk assessment and preoperative employed. Dr. Fisher discussed some
Preoperative consultations are commonly management of medications in patients of the benefits and limitations of risk
conducted for patients undergoing
undergoing non-cardiac surgery.
assessment tools, which are summarized
major non-cardiac surgery. This task
in the table on the opposite page.
involves risk stratification, risk reduction, Several cardiac risk stratification tools
are available, among which the ASA
Risk assessment tool Benefits
ASA physical status
• Widely used and
• Not explicitly developed as a risk assessment tool
classification system
• Clinical acumen required
• Derived in a non-contemprary patient population
• Derived from a large,
• Becoming "stale" (developed 12 years ago)
prospective study
• Underestimates risk
• Widely used and
• Included only two types of surgical patients (does not reflect
orthopedic population)
• Does not predict vascular risk very well
VSG-CRI (Vascular Study • Recently developed
• Complicated model
Group of New England – (2010)
Cardiac Risk Index)
• Derived from a large
• Limited utility for internists who are less likely to consult on
vascular surgery patients
rCRI (Erasmus model)
• Stratifies risk by age
• ROC increased from
Cardiac Risk Calculator
• Recently developed (2011) • Not a research trial
• Derived from a large
• No preoperative and postoerative evaluations
database of 250,000
• Average age of cohort 10 years younger than rCRI cohort
• Only included hard cardiac endpoints (MI and cardiac arrest)
• Medical chart review
• 1/3 were low risk surgeries (laparoscopy, breast surgery)
with high quality data
not normally candidates for preoperative consultation
• ASA classification embedded in the score (i.e., "a model within a model")
• Low sensitivity
ROC: receiver-operator curve
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Dr. Fisher noted that the simple and
that it is not "ready for prime time" yet.
A sensitivity analysis showed that risk
rapid Ankle-Brachial Index (ABI) correlates
More definitive data on how to make use of was increased only when the consultation
well with the rCRI, and is probably
this biomarker is eagerly awaited from the
was carried out by specialists rather than
worth doing to ensure a patient does
ongoing VISION trial, with results expected generalists and when the consultation
not have undeclared vascular disease.
was within 7 days of surgery, suggesting
Among the newer tools and tests on the
Dr. Fisher concluded his workshop by
a narrower focus of the consultation and
horizon to improve risk stratification is
reviewing data from a retrospective cohort more aggressive interventions close to
brain natriuretic peptide (BNP). While
study that evaluated outcomes in more
surgery may increase the risk for harm
studies to date suggest this easy-to-
than 270,000 patients undergoing major
to patients. Dr. Fisher concluded that
measure biomarker may offer additional
elective non-cardiac surgery in Ontario
"Before you do stuff, you should ask
prognostic information for mortality and
from 1994 to 2004. In this cohort, 39% of
yourself what you'll do with the results,
cardiac events after major non-cardiac
patients had a preoperative consultation
and give yourself enough time to have
surgery, this benefit is offset by the lack
at a median of 15 days prior to surgery.
the intervention work." For example,
of understanding regarding what to do
Using matched propensity analysis, the
smoking cessation often takes longer than
with the information. Furthermore, there
investigators showed that patients who
2 weeks, beta-blocker initiation within
has been substantial variability between
received preoperative risk assessment and 1-2 weeks of surgery can be dangerous,
studies evaluating BNP and pro-BNP (e.g.,
management had higher 30-day and 1-year and statins require several weeks to have
types of surgeries, patients' risk level,
mortality, longer hospital stay, increased
an appreciable effect on blood lipids.
mortality rates, etc.) and a threshold BNP
preoperative testing and pharmaceutical
"As advocates for our patients, we need
level has yet to be defined. While BNP may
interventions, compared to patients who
to actively lobby to stop last-minute
be a tantalizing idea, Dr. Fisher concluded
did not receive a preoperative consultation. management strategies."
it for communication between
increased in magnitude when
physicians. Perhaps more impactful
only consultations performed by
Dr. Fisher pointed out that several
was his discussion of the paper by
specialists or within 1 to 7 days
of the tools used to predict patient
Duminda et al (Arch Intern Med
of surgery were considered." This
risk in the perioperative period
2010;170:1365-74). The discussion
suggests that the last minute pre-
were not developed for that
of that paper points out that: "In
operative consultation achieves little
purpose, but rather to categorize
sensitivity analyses, the association
benefit and interventions may carry
of consultation with mortality was
more risk than benefit.
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Please join us at the 2012 CSIM Annual Scientific Meeting.
2012 CSIM Annual Scientific Meeting
In collaboration with ASMIQ
October 17-20, 2012 - Quebec City, QC
Program and registration information will be posted at www.csimonline.com
For more information please contact [email protected]
Please join us at the 2012 Rocky Mountain Conference of General Internal Medicine.
2012 Rocky Mountain Conference
November 22-25, 2012 - Banff Park Lodge, Banff AB
Program and registration information will be posted at www.rockymountaininternalmed.com
1-3170 Ridgeway Dr, Mississauga ON, L5L 5R4
P 905 607 4201 F 905 607 3163
www.evidencebasedmarketing.ca
CONFIDENTIAL - Distribution or use of this document and the contents is
prohibited without the express written permission of EBM Consulting Inc.
Source: http://www.evidencebasedmarketing.ca/images/downloads/RCMTN_V4_14JUN2012.pdf
P.O.Box 2345, Beijing 100023,China World J Gastroenterol 2003;9(10):2344-2347Fax: +86-10-85381893 World Journal of Gastroenterology E-mail: [email protected] www.wjgnet.com Copyright © 2003 by The WJG Press ISSN 1007-9327 • BRIEF REPORTS • Rapid and high throughput detection of HBV YMDD mutants withfluorescence polarization Yui-Jie Bai, Jin-Rong Zhao, Guan-Ting Lv, Wen-Hong Zhang, Yan Wang, Xiao-Jun Yan
Indonesia (see also ) Abused domestic worker is homeAn Indonesian domestic worker, Ceriyati Dapin, 33, who fled from her abusive Malaysian employer, was reunited with her family on 22 June. Indonesian Foreign Ministry spokesman Kristiarto Legowo said that the government would facilitate her trip back to Malaysia to pursue her legal case. Malaysian police have arrested the employer and charged her with unlawful confinement and causing injury with a dangerous weapon. Following the incident, Indonesia and Malaysia have agreed to revise the MOU on migrant workers. Both countries will form a committee to revise the articles to ensure better working conditions for Indonesian workers in Malaysia. Indonesian Minister for Manpower and Transmigration Eman Suparno argued that the provision permitting employers to hold the passports of workers in the informal sector render workers vulnerable and increases their risk of detention during immigration raids. According to data from the Ministry of Manpower and Transmigration, Indonesia deployed some 3.9 million workers, with as many as 1.2 million going to Malaysia. Migrant workers should keep their passportsParticipants in a seminar on human trafficking, organized by the US Embassy, agreed that Indonesian workers abroad are abused because they do not have their passports with them. There are some 1.2 million regular and 500,000 irregular Indonesian workers in Malaysia. Endang Sulistyaningsih, director of promotion at the National Agency for the Placement and Protection of Indonesian Overseas Workers, said that the government asked the Malaysian government to permit Indonesian workers to keep their passports at a renegotiation of the bilateral MOU on migrant workers in Surabaya on 28 and 29 June. Also under discussion are a wage raise, a day off, and basic requirements employers should meet, such as no criminal record and a certain income level. Wahyu Susilo, founder of Migrant Care, said that Malaysia would not be able to meet Indonesia's demand for workers to keep their passports because Malaysia's law stipulates that employers must keep their workers' passport. Indonesians arrested in the USOn 19 June, US immigration authorities arrested 81 irregular immigrants – 76 Indonesians and four Malaysians – at Iridium Industries Inc., a plastics factory in Pennsylvania. Iridium's plant manager, Wayne Migliaccio, said his company uses several recruitment agencies and it is their responsibility to check workers' immigration status. The Indonesian government has demanded access to the Indonesian migrants 76 Indonesians to ensure that they get legal assistance, said a Foreign Ministry spokesman Kristiarto Legowo. The workers allegedly overstayed their visas. 3 Indonesians to be deportedThree irregular Indonesian workers, identified as Bambang Heri, Lestari Budiman and Hans Woworuntu, currently detained at the Lackawanna County detention center, Pennsylvania are to be deported. They arrived in the US in 2000 and were arrested in April this year. Another Indonesian, identified as Suratman, is still consulting his lawyer on whether he would accept deportation or try to extend his stay permit in the US. Indonesian in US detention drugged for deportationTwo immigrants, from Indonesia and Senegal, claiming they were forcibly drugged for deportation sued the US Department of Homeland Security. The American Civil Liberties Union of Southern California filed the suit, demanding a federal court prohibit authorities from drugging deportees taking commercial flights unless a physician prescribes it is necessary. Raymond Soeoth, a 38-year-old Indonesian, was given the drugs Haldol and Cogentin in December 2004 at a Los Angeles detention center. The organization filed the suit said he had no history of mental illness and was not examined by a doctor before being drugged. Deported migrants maltreated by authorities at home



