Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Layout

Intratympanic Therapy inMeniere's Disease
Mr Simon Lloyd,
Consultant
Neuro-otologist,
University Department
of Otolaryngology,
Central Manchester NHS
Foundation Trust,
Oxford Road,
The principle of delivering a drug to the middle ear through the tympanic
membrane is not new with reports in the literature from the nineteenth
century regarding its efficacy as a treatment for ‘catarrhal affections of the
middle ear'.1,2 However, the use of this techniquein the treatment for inner ear disorders
Manchester, M13 9WL, UK.
has only been popularised over the past 20 years particularly in treating Meniere's
Disease and more latterly sudden sensorineural hearing loss. This article focuses on
Email: [email protected]
intratympanic therapies used in the treatment of Meniere's Disease.
Declaration of
Competing Interests
None declared.
Current delivery methods
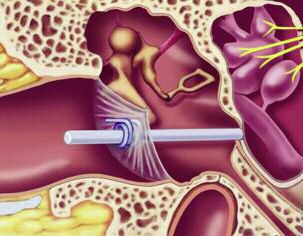
sponge running through the central passage
Intratympanic therapies aim to deliver a
and this can be slid down to come in to
given pharmacological agent to the inner ear
contact with the round window niche.
via the tympanic cavity and in so doing opti-
Drugs can then be delivered into the
mise inner ear dosage and reduce the risk of
external ear canal and they soak the sponge
developing systemic side effects. However,
and diffuse down to the middle ear (Figure
delivery of drugs to the inner ear is chal-
lenging. Systemic delivery has significant limi-
Some authors have also described the use
tations with variable penetration due to the
of fine catheters placed adjacent to the
presence of a blood-inner ear barrier as well
round window membrane via the tympanic
the risk of significant side effects. Similarly,
membrane in order to allow prolonged or
more direct access to the inner ear is limited
repeated drug delivery. Pump systems that
because the structures within the labyrinth
may be either partly or fully implantable may
are contained within hard bone and are only
be used to deliver the drug. However, this
accessible through the middle ear via the
technique is associated with a high propor-
round and oval windows. Access is made all
tion of complications, particularly accidental
the more difficult by the fact that minor
dislocation of the catheter, and has not
trauma to the membranous structures of
entered widespread use in clinical practice.
the inner ear can result in acute labyrinthinefailure. In addition, there are a number of
Current intratympanic drug
potential drawbacks to current intratym-
treatments in Meniere's Disease
panic drug delivery strategies including loss
There are currently two main groups of drug
of drug down the Eustacian tube as well as
used to treat Meniere's Disease via the
poorly understood intracochlear pharmaco-
intratympanic route. They are aminoglyco-
kinetics. Some have also expressed concern
side antibiotics and steroids.
regarding poor absorption of drug throughthe round window. However, a recent study
by Bird et al. has suggested that the dose
Aminoglycoside antibiotics, particularly
delivered to the cochlea following intratym-
gentamicin, are commonly used to treat
panic therapy is 260 times greater than the
gram negative bacterial and some types of
dose delivered by intravenous therapy.3
mycobacterial infection. One of their side
There are a number of different methods
effects is ototoxicity and this is the basis for
of delivering drugs intratympanically.4 The
their use in Meniere's Disease.
most common method of intratympanic
Most are predominantly cochleotoxic,
drug delivery is injection through the
resulting in sensorineural hearing loss in a
tympanic membrane (Figure 1). A typical
significant proportion of patients. However,
regimen for this type of administration is
gentamicin is predominantly vestibulotoxic
shown in Figure 2.
and is less likely to result in hearing loss.
An alternative method of drug delivery is
The mechanism of toxicity is unclear.
the Silverstein wick.5 This consists of a
From pathology studies it would appear that
grommet that is inserted into the eardrum in
they induce hair cell death within the
the posteroinferior quadrant over the round
cochlea at high doses.6 There is probably a
window niche. The grommet has a porous
preference for outer hair cells. At lower does,

they appear to damage the stereocilia ofboth cochlea and crista sensory cells.7 Theyprobably also have a damaging effect on theotolithic hair cells although this may be lesssignificant. The mechanism by which thesechanges are produced is not completelyclear. Aminoglycosides are actively trans-ported into cells where they bind to iron.
This may then form a toxic metabolite thatgenerates free radicals resulting in cellularinjury and cell death.8 There may also be aneffect mediated through a reduction inmitochondrial protein production and an
associated reduction in ATP production.
This is an attractive hypothesis given thatmitochondria have many similarities to
A protocol for the administration of intratympanic gentamicin
The first description of the use of amino-
The following procedure can be performed in an out patient setting
glycosides via the intratympanic approach
Mix the following in a 2ml syringe:
was by Schuknecht in 1956. He used strep-
• 1.5mls of 80mg/ml gentamicin
tomycin.9 However, this drug was associatedwith a very high incidence of sensorineural
• 0.3mls of water for injection
hearing loss because of its ototoxicity. As a
• 0.2mls of 84mg/ml sodium bicarbonate
result the popularity of intratympanic injec-tion of aminoglycosides waned until it
Place the patient supine with the head flat and turned away from the ear to be
became clear that gentamicin was equally
injected. Use topical anaesthetic agents such as EMLA or Ametop to anaesthetize
effective at resolving symptoms but was less
the tympanic membrane
Under the operating microscope, inject the buffered gentamicin through the tym-
There are several papers evaluating the
panic membrane in the posteroinferior quadrant just over the round window niche
efficacy of intratympanic gentamicin in
using a spinal needle. The middle ear can be seen to fill up with the fluid
Meniere's Disease. Unfortunately, the study
Leave the patient supine with their head turned away for 40 minutes. The patient
design and protocols for administration vary
may feel some of the drug pass down the Eustacian tube into the nasopharynx
widely and this makes comparison of
Repeat injections weekly until they start to experience imbalance as a result of the
outcomes difficult. Some investigate high
treatment, their symptoms resolve or if there is a deterioration in their hearing. This
dose single injection therapy. Others investi-
is usually 2-3 injections
gate staged, lower dose administration. This
Some clinicians prefer to insert a ventilation tube at the time of the first injection
may be given daily, weekly or monthly.
in order to avoid the need to facilitate subsequent injections
Similarly, the end point of treatment varies.
This may be the rendering of the labyrinthavestibular or the onset of vestibular symp-toms. Onset of hearing should also triggercessation of therapy.
All studies suggest that intratympanic
gentamicin is an effective treatment forvertigo in Meniere's Disease but treatmentmust balance the need to control symptomswith the potential for cochleotoxicity. Thedosage of gentamicin used varies in the liter-ature from 2.4 to 720mg. The effectiveness ofintratympanic gentamicin in completelyresolving vertigo symptoms in Meniere'sDisease varies from 27% to 100% dependingon the series.10-15 A meta-analysis of 27studies by Chia et al. found that the meancomplete vertigo control rate for all types ofregimen was 73.6%.16 Low dose staged treat-ments controlled vertigo completely (AAOvertigo score of 0) in 66.7% of cases. Theeffective vertigo control rates (AAO vertigoscore of 1-40) were 90.2% and 86.8% respec-tively for all regimens and low dose regimens.
The risk of hearing loss (partial and
profound) ranged from 0% to 90% but
subject to the same limitations of
adhesions or round window thickening in
the mean hearing loss for all regimens was
heterogenous study design.
those who fail this form of therapy. In this
25.1% with low dose regimens producing
Intratympanic steroids appear to be
situation exploration of the middle ear to
hearing loss in 13.1%. A recent Cochrane
effective in controlling vertigo in
improve access to the round window
reviewhas further assessed the literature17
Meniere's Disease but they are probably
followed by direct placement of gentam-
and found only two well designed
less efficacious than gentamicin. The liter-
icin on a pledget onto the round window
randomised placebo controlled trials.10,11
ature would suggest that 41-82% of
resolves symptoms in the majority of
The first study by Stokroos et al.
patients have complete relief of vertigo
initial treatment failures.30
suggested that there was a complete
and 72-91% of patients have adequate
resolution of vertiginous symptoms in all
control of their vestibular symptoms
When to use intratympanic therapy
patients and that this was significantly
following treatment. More than four
Intratympanic treatment with gentamicin or
greater than placebo. They had no signifi-
injections may be required in some cases
steroid has become the first line of treat-
cant hearing deterioration in any patient.
and a proportion require further injec-
ment following failure of conservative
The second study by Postema et al.
tions a few months after the original
management in Meniere's Disease. This is
showed that vertigo scores reduced from
treatment.23-27 Most studies suggest that
because of the documented effectiveness of
2.1 to 0.5 in the gentamicin group
hearing is not affected in either a positive
these drugs and because of the simplicity
compared to 2.0 to 1.8 in the placebo
or negative way following steroid injec-
and safety of the procedure. However, there
group. Average hearing loss in the
are very few studies comparing outcomes of
gentamicin group was 8.1dB compared to
There have been no meta-analyses
these two types drug. Sennaroglu et al. have
0dB in the placebo group.
performed investigating the efficacy of
shown effective vertigo control in 72% of
From the literature, it would appear
intratympanic steroid in Meniere's
patients with intratympanic dexametha-
that a dose of 30mg/ml administered
Disease to date. However, a Cochrane
sone, 75% of patients with intratympanic
weekly with end points of resolution of
review has been performed by Phillips
gentamicin and 52% for endolymphatic sac
symptoms, onset of vestibular symptoms
and Westerberg.28 They felt that only one
surgery.24 Other studies are on going
because of treatment or onset of hearing
randomised placebo controlled trial met
(Bronstein et al. unpublished).
loss provides the most effective method
rigorous criteria regarding quality. This
The decision to use gentamicin or
of symptom control with the lowest risk
paper, published by Garduno-Anaya et al.,
steroid is dependent on the amount of
of hearing impairment.16,18,19 This may be
showed that intratympanic 4mg/ml
hearing remaining in the ear to be treated
buffered with 84% sodium bicarbonate in
Dexamethasone was an effective treat-
and on the status of the opposite ear. If
order to reduce discomfort during injec-
ment in improving vestibular symptoms
there is serviceable hearing in the ear to
tion. Between one and four injections
in Meniere's Disease.27 Eighty-two per
be treated and the opposite ear has
may be required to achieve symptom
cent of the steroid group achieved
poorer hearing or evidence of significant
control and further injections may be
complete control of symptoms (AAO
vestibular impairment then steroid is the
required in the future. A typical regimen
class A) compared to 57% in the placebo
drug of choice as it is unlikely to render
is shown in Figure 1. For low dose treat-
group. There was no significant change in
the patient deaf or avestibular. If the ear
ments, the time taken until further injec-
hearing. There was no significant change
to be treated has poor hearing and the
tions are required to control recurrent
in tinnitus.
opposite ear is healthy then gentamicin is
vestibular symptoms may be in the region
A number of different steroids have
the drug of choice. However, it is impor-
of four months.20
been used in Meniere's Disease. The most
tant to bear in mind that around 20% of
With regards to modification of other
commonly used are dexamethasone and
patients will develop Meniere's Disease in
Meniere's symptoms, most studies have
methylprednisalone. Doses are very vari-
the opposite ear at some point.
found that intratympanic gentamicin
able between studies. For example
does not modify tinnitus but may reduce
dexamethasone doses vary between
symptoms of aural fullness.10,11
1mg/ml and 19mg/ml. Pain may be trou-
There are a number of papers that have
blesome following injection although this
investigated the response of fluctuating
seems to be less of an issue for dexam-
sensorineural hearing loss seen in
Intratympanic steroid injections have
ethasone. A dose of 4mg/ml of dexam-
cochlear hydrops to intratympanic
become increasingly popular as a means
ethasone would seem reasonable based
steroid injection. The proportion of
of controlling vestibular symptoms in
on the literature.
patients who have an improvement in
Meniere's Disease. They have the poten-
As with gentamicin, it would appear
their hearing is lower than the proportion
tial advantage over gentamicin of not
that intratympanic steroids do not signif-
of patients that get an improvement in
being inherently ototoxic. They are
icantly modify tinnitus associated with
their balance symptoms and ranges from
thought to act through an anti-inflamma-
Meniere's Disease.29
40 to 74% depending on the series.31,32
tory effect but may also have an influence
Care must be taken when interpreting
on sodium and fluid transport within the
Failure of intratympanic
this data however, as by its very nature
the hearing loss is fluctuating and
Steroids delivered intratympanically-
It remains unclear why some patients do
certainly a significant proportion may
have been used to treat Meniere's
not respond to intratympanic therapy
have improved spontaneously without
Diseasesince the early 1990s.22 However,
but there is some evidence that it may
intervention. Nevertheless, intratympanic
the literature regarding intratympanic
reflect ineffective delivery of drug in a
steroid injection should be considered for
steroids in Meniere's Disease is less exten-
significant proportion of cases. Some
the management of acute hearing loss
sive than that for gentamicin and is
authors have noted a high incidence of
resulting from cochlear hydrops.
The future of intratympanic therapy
Drug delivery systems
1. Bronner A. On intratympanic injections in the treat-
21. Trune DR, Kempton JB, Kessi M. Aldosterone (miner-
Given the challenges of access to the inner
ment of chronic dry catarrh of the middle ear. Br
alocorticoid) equivalent to prednisolone (glucocorti-
Med J 1894;2(1763):805.
coid) in reversing hearing loss in MRL/MpJ-Fas1pr
ear, a number of techniques are currently
autoimmune mice. Laryngoscope 2000;110:1902-6.
being developed for the delivery of drugs
2. Weber-Liel. On intratympanic injections in catarrhal
affections of the middle ear. Br Med J
22. Itoh A, Sakata E. Treatment of vestibular disorders.
not just via the middle ear but directly to
Acta Otolaryngol Suppl 1991;481:617-23.
the inner ear.
3. Bird PA, Murray DP, Zhang M, Begg EJ. Intratympanic
23. Boleas-Aguirre MS, Lin FR, Della Santina CC, Minor
Microcatheters that deliver drugs
versus intravenous delivery of dexamethasone and
LB, Carey JP. Longitudinal results with intratympanic
directly into the inner ear are currently
dexamethasone sodium phosphate to cochlear peri-
dexamethasone in the treatment of Ménière's dis-
lymph. Otol Neurotol 2011;32(6):933-6.
ease. Otol Neurotol 2008;29(1):33-8.
under development. These have been used
4. McCall AA, Swan EE, Borenstein JT, Sewell WF,
24. Sennaroglu L, Sennaroglu G, Gursel B, Dini FM.
in conjunction with pump systems such
Kujawa SG, McKenna MJ. Drug delivery for treat-
Intratympanic dexamethasone, intratympanic gen-
as osmotic pumps or reciprocating perfu-
ment of inner ear disease: current state of knowl-
tamicin, and endolymphatic sac surgery for
edge. Ear Hear 2010;31(2):156-65.
intractable vertigo in Meniere's disease. Otolaryngol
Head Neck Surg 2001;125:537-43.
One of the primary limitations of
5. Silverstein H, Jackson LE, Rosenberg SI. Silverstein
Microwick for treatment of inner ear disease. Oper
25. Hirvonen TP, Peltomaa M, Ylikoski J. Intratympanic
current intratympanic therapy tech-
Tech Otolaryngol Head Neck Surg 2001;12:144–147.
and systemic dexamethasone for Meniere's disease.
niques is the limited exposure that the
ORL J Otorhinolaryngol Relat Spec 2000;62:117-20.
6. Polgar R, Collison T, Slepecky NB, Wanamaker HH.
round window has to the drug being
Anatomic and morphometric changes to gerbil pos-
26. Barrs DM, Keyser JS, Stallworth C, McElveen JT.
delivered because of its low viscosity.
terior cristas following transtympanic administration
Intratympanic steroid injections for intractable
of gentamicin and streptomycin. JARO 2001;2:147-58.
Meniere's disease. Laryngoscope 2001;111:2100-4.
Hydrogels that can be loaded with a drugand placed over the round window have
7. Oei ML, Segenhout HM, Dijk F Stokroos I, van der
27. Garduno-Anaya MA, Couthino De Toledo H,
Want JJ, Albers FW. Functional and anatomic alter-
Hinojosa GR, Pane PC, Rios Castaneda LC.
been demonstrated to improve exposure
ations in the gentamicin-damaged vestibular system
Dexamethasone inner ear perfusion by intratympan-
to the round window by maintaining
in the guinea pig. Otol Neurotol 2004;25(1):57-64.
ic injection in unilateral Meniere's disease: a two-yearprospective, placebo-controlled, double- blind, ran-
contact with the drug for a prolonged
8. Song BB, Anderson DJ, Schacht J. Protection from
domized trial. Otolaryngol Head Neck Surg
gentamicin toxicity by iron chelators in guinea pig in
vivo. J Pharmacol Exp Th 1997;282(1):369-77.
Vectors such as viral particles or
28. Phillips JS, Westerberg B. Intratympanic steroids for
9. Schuknecht HF. Ablation therapy for the relief of
nanoparticles are showing promise as
Ménière's disease or syndrome. Cochrane Database
Meniere's disease. Laryngoscope 1956;66:859-70.
Syst Rev 2011;6(7).
techniques for delivering drugs into the
10. Postema RJ, Kingma CM, Wit HP, Albers FW, Van
inner ear.35 The particles can be filled
29. Silverstein H, Choo D, Rosenberg S, Kuhn J, Seidman
Der Laan BF. Intratympanic gentamicin therapy for
M, Stein I. Intratympanic steroid treatment of inner
with a ‘cargo' such as a drug or gene
control of vertigo in unilateral Meniere's disease: a
ear disease and tinnitus (preliminary report). Ear
prospective, double-blind, randomized, placebo-con-
plasmid and injected into the middle or
Nose Throat J 1996;75:468-71.
trolled trial. Acta Otolaryngol 2008;128(8):876-80.
inner ears. Their delivery to a specific site
30. Crane BT, Minor LB, Della Santina CC, Carey JP.
11. Stokroos R, Kingma H. Selective vestibular ablation
can be facilitated by the addition of
Middle ear exploration in patients with Ménière's
by intratympanic gentamicin in patients with unilat-
disease who have failed outpatient intratympanic
ligands to their surface that aid in trans-
eral active Meniere's disease: a prospective, double-
gentamicin therapy.Otol Neurotol 2009;30(5):619-24.
blind, placebo- controlled, randomized clinical trial.
membrane transport or binding to the
31. Selivanova OA, Gouveris H, Victor A, Amedee RG,
target tissue.
Mann W. Intratympanic dexamethasone and
12. De Stefano A, Dispenza F, De Donato G, Caruso A,
hyaluronic acid in patients with low-frequency and
Taibah A, Sanna M. Intratympanic gentamicin: a 1-
Ménière's-associated sudden sensorineural hearing
day protocol treatment for unilateral Meniere's dis-
loss. Otol Neurotol 2005;26(5):890-5.
ease. Am J Otolaryngol 2007;28(5):289-93.
In addition to steroids and gentamicin,
32. Hillman TM, Arriaga MA, Chen DA. Intratympanic
therapeutic agents for inner ear disease
13. Quaranta A, Scaringi A, Aloidi A, Quaranta N,
steroids: do they acutely improve hearing in cases of
Salonna I. Intratympanic therapy for Meniere's dis-
currently under investigation include
cochlear hydrops? Laryngoscope 2003;113(11):1903-
ease: effect of administration of low concentration
anti-oxidants that may confer a protec-
of gentamicin. Acta Otolaryngol 2001;121(3):387-92.
33. Sewell WF, Borenstein JT, Chen Z, Fiering J, Handzel
tive effect in the prevention of noise
14. Silverstein H, Arruda J, Rosenberg SI, Deems D, Hester
O, Holmboe M, Kim ES, Kujawa SG, McKenna MJ,
induced hearing loss,36 neurotrophins
TO. Direct round window membrane application of
Mescher MM, Murphy B, Swan EE, Peppi M, Tao S.
gentamicin in the treatment of Meniere's disease.
such as neurotrophin-3 that may stimu-
Development of a microfluidics-based intracochlear
Otolaryngol Head Neck Surg 1999;120(5):649-55.
drug delivery device. Audiol Neurootol
late regeneration of cochlear nerve fibres
15. Delgado LP, Rodrigo JF, Pena PA. Intratympanic gen-
or hair cells,37 genes that could be spliced
tamicin in Meniere's Disease: our experience. J
34. Borden RC, Saunders JE, Berryhill WE, Krempl GA,
into the genome of inner ear cells to stim-
Thompson DM, Queimado L. Hyaluronic acid
ulate the production of a deficient
16. Chia SH, Gamst AC, Anderson JP, Harris JP.
hydrogel sustains the delivery of dexamethasone
Intratympanic gentamicin therapy for Meniere's dis-
across the round window membrane. Audiol
protein product38 and stem cell therapies.
ease: a meta-analysis. Otol Neurotol 2004;25(4):544-
35. Poe DS, Pyykko I. Nanotechnology and the treat-
17. Pullens B, van Benthem PP. Intratympanic gentamicin
ment of inner ear diseases. WIREs Nanomed
Current intratympanic therapies are
for Ménière's disease or syndrome. Cochrane
Database Syst Rev 2011;16(3).
effective in treating a significant propor-
36. Kopke RD, Wassel RA, Mondalek F,Grady B,Chen K,
tion of patients with Meniere's Disease.
18. Carey J. Intratympanic gentamicin for the treatment
Liu J, Gibson D, Dormer KJ. Magnetic nanoparticles:
of Meniere's disease and other forms of peripheral
inner ear targeted molecule delivery and middle ear
Gentamicin is probably more effective
vertigo. Otolaryngol Clin North Am 2004;37(5):1075-
implant. Audiol Neurootol 2006;11:123-33.
than steroids but has a small risk of
37. Tessarollo L, Coppola V, Fritzsch B. NT-3 replacement
inducing sensorineural hearing loss. There
19. Beck C, Schmidt CL. 10 years of experience with
with brain-derived neurotrophic factor redirects
are many new drug delivery systems and
intratympanally applied streptomycin (gentamycin)
vestibular nerve fibers to the cochlea. J Neurosci
in the therapy of Morbus Meniere. Arch
pharmacological agents under develop-
38. Izumikawa M, Minoda R, Kawamoto K, Abrashkin
ment and these may result in the ability
20. Nguyen KD, Minor LB, Della Santina CC, Carey JP.
KA, Swiderski DL, Dolan DF, Brough DE, Raphael Y.
to prevent and even reverse Meniere's
Time course of repeated intraytympanic gentamicin
Auditory hair cell replacement and hearing improve-
Disease in the future. n
for Meniere's Disease. Laryngoscope 2009;119(4):792-
ment by Atoh1 gene therapy in deaf mammals. Nat
Source: http://earandhearing.co.uk/wp-content/uploads/2015/05/IT-therapy-in-Menieres-Disease.pdf
Heft 26 6. Jahrgang u Gefahr auf der Weide Eine vorbeugende Parasitenbehandlung sichert zwangsläufig nicht nur die Gesund-heit und Leistungsfähigkeit der Rinder sondern auch den wirtschaftlichen Ertrag. Außerdem verursacht ein Parasitenbefall weitere unnötige Kosten. Demgegenüber stehen im ökologischen Landbau die Ansprüche an eine Minimie-rung des Tierarzneimitteleinsatzes und die damit verbundenen Risiken. Aber auch in ökologisch bewirtschafteten Betrieben ist eine Kontrolle des Parasitenbefalls der Weidetiere zur Erhaltung der Tiergesund-heit unabdingbar, da eine ökologische Fütterung und Haltung allein zur Vorbeu-gung und Bekämpfung eines Parasiten-befalls nicht ausreichen.
The Analysis of Estrogens Using Liquid Chromatography and Negative Electrospray Ionization Mass SpectrometryKatie estridge1,2, carol Babyak2, wendy lewis2 1environmental science Program, appalachian state University, Boone, nc 2a.R. smith department of chemistry, appalachian state University, Boone, nc [email protected]



