Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
No job name
British Journal of Clinical
Correspondence
Dr Geoff Isbister, Department of Clinical
Toxicology, Calvary Mater Newcastle
and arrhythmias in
Hospital, Edith St, Waratah, NSW 2298,Australia.
Tel: + 612 4921 1211
venlafaxine overdose
Fax: + 612 4921 1870E-mail: geoffrey
Geoffrey K. Isbister
arrhythmia, cardiac toxicity, overdose, QRSwidth, QT prolongation, venlafaxine
Menzies School of Health Research, Charles Darwin University, Darwin and Department of Clinical
Toxicology and Pharmacology, Calvary Mater Newcastle Hospital, Waratah, Australia
Received
13 October 2008
Accepted
14 January 2009
WHAT IS ALREADY KNOWN ABOUT
THIS SUBJECT
• The major clinical effects of venlafaxine
overdose are seizures and serotonin toxicity.
• There is controversy over the risk of cardiac
To investigate serial electrocardiogram (ECG) parameters,
toxicity in venlafaxine overdose.
haemodynamic changes and arrhythmias following venlafaxineoverdose.
WHAT THIS STUDY ADDS
The study included 369 venlafaxine overdoses in 273 patientspresenting to a toxicology unit where an ECG was available.
• Venlafaxine overdose is unlikely to cause
Demographic information, details of ingestion, haemodynamic effects
clinically significant cardiac toxicity,
[heart rate and blood pressure (BP)] and complications (arrhythmias
including QT prolongation or malignant
and conduction defects) were obtained. ECG parameters (QT, QRS) were
arrhythmias, and the commonest
measured manually and analysed by visual inspection, including
cardiovascular effects are tachycardia and
plotting QT–HR pairs on a QT nomogram.
mild hypertension.
• Massive ingestions >8 g may result in
The median ingested dose was 1500 mg [interquartile range (IQR)
cardiac toxicity and patients should be
600–3000 mg; range 75–13 500 mg). Tachycardia occurred in 54%
observed carefully.
and mild hypertension (systolic BP >140 mmHg) in 40%. Severehypertension (systolic BP >180 mmHg) and hypotension (systolic BP
<90 mmHg) occurred in 3% and 5%, respectively. No arrhythmiasoccurred based on continuous telemetry, and conduction defects werefound in only seven of 369 admissions; five of these conduction defectswere pre-existing abnormalities. In 22 admissions [6%, 95% confidenceinterval (CI) 4–10] there was an abnormal QT–HR pair, with larger dosesbeing more likely to be associated with an abnormal QT. The medianmaximum QRS width was 85 ms (IQR 80–90 ms; range 70–145 ms) andthe QRS was greater than 120 ms in only 24 admissions (7%, 95% CI4–10).
CONCLUSIONS
Venlafaxine overdose causes only minor abnormalities in the QT and
QRS intervals, unlikely to be associated with major arrhythmias, except
possibly with large doses.
than other newer antidepressants, with a higher rate offatalities [1], increased risk of seizures [2] and cardiac tox-
Many of the newer antidepressants have been shown to be
icity reported with massive ingestions [3]. Serotonin toxic-
safer in overdose compared with the older tricyclic antide-
ity and seizures are the most important clinical effects
pressants. However, venlafaxine appears to be more toxic
commonly reported following venlafaxine overdoses and
Br J Clin Pharmacol
2009 The Author
Journal compilation 2009 The British Pharmacological Society
occur across a range of doses. Cardiac effects are rare,
All patients presenting with drug overdose are either
being reported with massive ingestions, and are not well
managed in the Emergency Department (ED) by the toxi-
cology unit, if their length of stay is less than about 16 h, or
A recent report of venlafaxine overdoses has suggested
admitted as an inpatient under toxicology if they require
that cardiac toxicity is more common and is associated
intensive care admission or a longer duration of stay. All
with abnormal QT prolongation. The study concluded that
toxicology admissions have continuous telemetry while in
QT prolongation is a major problem with venlafaxine over-
the ED and therefore a large proportion of patients will
dose and all patients require cardiac monitoring [6].
have continuous telemetry for the duration of their hospi-
However, this study by Howell
et al. focused on QT prolon-
tal stay. Because of the risk of seizures, patients with ven-
gation with single electrocardiograms (ECG) and used
lafaxine overdose that have an inpatient admission will
Bazett's correction where the majority of patients had
usually be admitted to the high dependency or intensive
tachycardia. They reported no serious arrhythmias and it is
care unit, which also have continuous telemetry. A minority
ultimately unclear what the potential is for clinically signifi-
of venlafaxine overdose patients being admitted for >16 h
cant cardiac toxicity in venlafaxine overdose. The sugges-
will be transferred to the general ward without telemetry.
tion that QT prolongation is the most important parameter
The toxicology service has a standardized discharge policy
is also inconsistent with previous reports, where QRS wid-
requiring review by the medical toxicology team and the
ening and sodium channel blockade may be the mecha-
psychiatry team. Both teams are available to perform
nism of cardiotoxicity in massive overdoses.
reviews on a 24/7 basis.
The aim of this study was to assess the effect of ven-
QT and QRS intervals were manually measured on each
lafaxine overdose on ECG parameters (QT interval, QRS
12-lead ECG with a ruler. The QT interval was taken from
width), blood pressure and heart rate, and determine the
the beginning of the Q wave up to the point where the T
frequency of arrhythmias.
wave returns to baseline. QT and QRS were measured in aminimum of six leads (three chest and three limb leads)and the median interval calculated. HR was recorded from
the ECG machine's automated readout and assumed to bean average measure of the RR interval for the ECG.This was
This study was a review of consecutive presentations of
confirmed in a subgroup of 57 patients where the RR inter-
venlafaxine overdose to a tertiary toxicology unit at the
val was measured from the same point in one complex to
Calvary Mater Newcastle Hospital (Australia), which has
the next complex for at least six RR intervals in the rhythm
a primary referral population of approximately 300 000
strip (lead II) and the median RR interval calculated and
people. Detailed information on all admissions is recorded
converted to HR.
in a relational database. The use of this database for
For descriptive statistics, medians and interquartile
research purposes has previously been exempted by the
ranges (IQR) are reported. ECG parameters were examined
Human Research Ethics Committee as an audit, and
by visual inspection, which included plotting QT–HR pairs
approval was obtained for prospective collection of clinical
on a previously developed QT nomogram [7] and plots of
data, blood samples and ECGs from a subgroup of patients.
QRS duration
vs. time and dose.
An earlier study has reported the first 51 venlafaxine over-dose admissions in a study of the relative toxicity of anti-depressants [2].
All venlafaxine overdoses between January 1997 and
December 2007 were reviewed and admissions where at
During the period of the study 317 patients presented on
least one ECG was available were included. The history of
436 occasions with venlafaxine overdoses. ECGs were avail-
venlafaxine ingestion was confirmed on at least two occa-
able for 273 patients on 369 occasions where the median
sions (history from ambulance officers, family, friends and
ingested dose was 1500 mg (IQR 600–3000 mg; range
empty drug containers) and blood was collected and ven-
75–13 500 mg). In a subgroup of 57 admissions where
lafaxine quantified in a subgroup of patients.The following
blood was collected, venlafaxine was detected in all cases.
information was extracted from the database: patient
Table 1 provides the demographic details and characteris-
demographic characteristics (age, sex), details of the inges-
tics for all 369 admissions where at least one ECG was
tion [estimated time of ingestion and amount (mg)],
available. Tachycardia was common, occurring in 54%
co-ingested drugs, clinical effects [heart rate (HR) and
of patients, as was mild hypertension (systolic BP
blood pressure (BP)] on admission and their respective rel-
>140 mmHg) occurring in 40%, but severe hypertension
evant maximum or minimum recordings during admission
(systolic BP >180 mmHg) and hypotension (systolic BP
and complications (arrhythmias and conduction defects).
<90 mmHg) were uncommon (Table 1).
Co-ingested drugs were classified as either having a signifi-
There were 663 ECGs available for the 369 admissions.
cant potential to cause QRS widening and/or QT prolonga-
An abnormal ECG (excluding sinus tachycardia) was found
tion based on both the drug and the dose ingested.
in seven of the 369 admissions, which were all conduction
Br J Clin Pharmacol
Table 1
Details of the 369 admissions from 273 patients reporting the median and interquartile range (IQR) or for dichotomous outcomes the number, percent
proportion and 95% confidence intervals (95% CI)
Median (IQR)
n =
273
n =
369
35 years (25–43)
Sex, female (%)
1.5 mg (0.6–3 g; range
Heart rate:
103 bpm (90–117)
Tachycardia (%) [HR >100 bpm]
199 (54% [49, 59])
138 mmHg (127–150)
Systolic BP >140 mmHg
149 (40% [35, 46])
Systolic BP >180 mmHg
Diastolic BP >110 mmHg
Systolic BP <90 mmHg
QT interval
360 ms (IQR 330–390 ms)
(Range 260–520 ms)
QRS width
85 ms (IQR 80–90 ms)
ⱖ120 ms
(Range 70–145 ms)
Abnormal ECG (%)
*Only two admission with QRS >120 ms (130 ms, 145 ms). IQR, interquartile range; BP, blood pressure.
defects (right bundle branch block [2], left anterior
overdose and the common cardiovascular effects are
hemiblock [3], right bundle branch block and left anterior
tachycardia and mild hypertension, consistent with it
hemiblock [1], first degree heart block [1]). In five of the
being a noradrenergic reuptake inhibitor. Malignant
seven cases with a conduction defect, it was a pre-existing
arrhythmias did not occur based on continuous telemetry.
ECG change based on previously recorded ECGs in the
Abnormal QT intervals and widening of the QRS interval
medical record. No arrhythmias were reported from con-
were uncommon, possibly associated with larger inges-
tinuous telemetry while in the ED or intensive care unit.
tions (>8 g), and were not grossly abnormal.
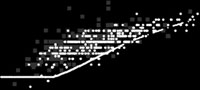
The most abnormal QT–HR pair for each of the 369
A previous study by Howell
et al. on the cardiovascular
admissions is plotted in Figure 1a on the QT nomogram,
toxicity of venlafaxine in overdose concluded that ven-
showing that in only 22 admissions (6%) was the QT–HR
lafaxine overdose is associated with a prolonged QTc and
pair above the line and therefore abnormal. Figure 1b illus-
this may pose an arrhythmogenic risk, despite no cases of
trates the QT nomogram for patients co-ingesting medica-
malignant arrhythmias occurring in their study [6]. There
tions reported to cause QT prolongation. Figure 1c,d
are also no published cases of venlafaxine overdose or
distinguishes the top and bottom 10th percentile of dose
ingestion being associated with torsades de pointes (TdP)
to explore the dose effect on QT. None of the patients
[7]. It is far more likely that the dose-dependent increase
ingesting a dose in the bottom 10% had an abnormal QT
in HR they report has simply translated into a dose-
compared with four (14%) in the top 10% of doses.
dependent over-correction of the QT interval using
Figure 1e compares the QT–HR pairs in venlafaxine with a
Bazett's formula [6]. Bazett's formula is known to be prob-
control group of overdoses of non-cardiotoxic medica-
lematic outside of the HR range 50–70 bpm [8], and ven-
lafaxine overdose results in a HR in the range where
The median maximum QRS width for the 369 admis-
Bazett's formula overcorrects. This is confirmed by the fact
sions was 85 ms (IQR 80–90 ms; range 70–145 ms), and in
that the reported absolute QT intervals in their study were
only 24 admissions was the QRS ⱖ120 ms (Table 1). There
not prolonged. This over-correction of the QT has previ-
was a poor and possibly no association between QRS and
ously been shown in other drugs that cause tachycardia in
dose, although QRS >120 ms occurred only for doses >5 g.
overdose such as quetiapine and bupropion [9, 10].
This study has shown that only a small proportion of
venlafaxine overdoses had an abnormal QT and these
cases were more likely to be larger ingestions (seeFigure 1c,d) or in patients who had co-ingested other
This study suggests that for the majority of cases, signifi-
drugs known to affect the QT interval (Figure 1b). The
cant cardiotoxicity does not occur with venlafaxine
overall pattern of the QT–HR pairs for venlafaxine over-
Br J Clin Pharmacol

val (msec) 400
val (msec) 400
100 120 140 160
100 120 140 160
Heart rate (bpm)
Heart rate (bpm)
val (msec) 400
val (msec) 400
100 120 140 160
100 120 140 160
Heart rate (bpm)
Heart rate (bpm)
val (msec) 350
100 120 140 160
Heart rate (bpm)
Figure 1
Plot of QT vs. heart rate (HR) in patients taking venlafaxine overdoses with one ECG for each patient (a).The nomogram line separates HR, QT pairs above the
line associated with an increased risk of torsades de pointes compared with those below the line [7]. (b) Shows patients co-ingesting drugs known to cause
QT prolongation in filled grey squares. (c) Shows patients taking the large doses (top 10%) in grey crosses and (d) has patients taking the smallest doses
(bottom 10%) in grey triangles. (e) Provides a comparison with a control group of patients taking overdoses of drugs that do not affect the QT interval [7]
in light grey squares
doses on the QT nomogram was only marginally differ-
venlafaxine toxicity, including seizures and serotonin tox-
ent from overdoses of non-cardiotoxic medications
icity [18], and there is a significant risk of death.
(Figure 1e). Figure 1 therefore provides good evidence that
There were a number of limitations of the study design,
QT prolongation is not a major feature of venlafaxine over-
including the fact that patient data were collected
dose, except possibly for larger overdoses, where the effect
prospectively and the ECGs reviewed retrospectively.
still remains moderate.This is in contrast to drugs that have
However, the haemodynamic parameters are objective
been clearly associated with QT prolongation and TdP
measures that are routinely collected in all toxicology
such as thioridazine [11], citalopram [12] and amisulpride
patients. ECGs were measured manually in a standardized
[13] and sodium channel effects well known to cause
way by the author using a previously published method
severe effects in tricyclic antidepressant poisoning [14].
[12]. Obtaining digitized ECG data using Holter monitors to
There have been previous reports of venlafaxine
record the 12-lead ECGs and on-screen measurement of
causing cardiac toxicity and death after large overdoses,
the QT intervals with magnification is more accurate [19].
consistent with our findings. There is one report of QRS
However, this was not possible because all the ECGs were
widening after an overdose of 3 g; however, the patient
recorded as hard copies. Automated measurement avail-
also ingested thioridazine [15]. There is one report of a
able on standard ECG machines is also inaccurate [19, 20],
hypertensive crisis that was associated with therapeutic
so was not used either.
venlafaxine use [16]. Other reports all include doses >8 g
Although all overdoses were not confirmed by mea-
[3–5, 17], where patients also manifest other features of
surement of venlafaxine in plasma, 100% of a subgroup
Br J Clin Pharmacol
of patients where blood was available for drug assays had
7 Chan A, Isbister GK, Kirkpatrick CM, Dufful SB. Drug-induced
venlafaxine in concentrations consistent with drug inges-
QT prolongation and torsades de pointes: evaluation of a QT
tion. There was also the possibility of inaccuracy in the
nomogram. QJM 2007; 100: 609–15.
dose from patient history. However, a number of pharma-
8 Hodges M. Rate correction of the QT interval. Card
cokinetic studies of drugs in overdose have demon-
Electrophysiol Rev 1997; 3: 360–3.
strated that patient estimate of dose is relatively accurate
9 Balit CR, Isbister GK, Hackett LP, Whyte IM. Quetiapine
[21, 22]. Therefore, patient estimate of dose is a reason-
poisoning: a case series. Ann Emerg Med 2003; 42: 751–8.
able pharmacokinetic metric to use in studies of effects indrug overdose.
10 Isbister GK, Balit CR. Bupropion overdose: QTc prolongation
and its clinical significance. Ann Pharmacother 2003; 37:
Venlafaxine remains a commonly prescribed antide-
pressant and will continue to be taken in overdose. Severecardiotoxicity with arrhythmias and/or hypotension does
11 Buckley NA, Whyte IM, Dawson AH. Cardiotoxicity more
not appear to be a major feature of venlafaxine overdose
common in thioridazine overdose than with other
except in massive ingestions of >8 g, when other features
neuroleptics. J Toxicol Clin Toxicol 1995; 33: 199–204.
such as neurotoxicity and serotonin toxicity are probably
12 Friberg LE, Isbister GK, Duffull SB.
more important. Routine cardiac monitoring is unlikely
Pharmacokinetic–pharmacodynamic modelling of QT
to be necessary in the majority of cases, but all patients
interval prolongation following citalopram overdoses.
should have at least one ECG.
Br J Clin Pharmacol 2006; 61: 177–90.
13 Isbister GK, Murray L, John S, Hackett LP, Haider T,
O'Mullane P, Gosselin S, Daly F. Amisulpride deliberateself-poisoning causing severe cardiac toxicity including QTprolongation and torsades de pointes. Med J Aust 2006; 184:
None to declare.
G.K.I. is funded by an NHMRC Clinical Career Development
14 Buckley NA, Dawson AH, Whyte IM, Henry DA. Toxicity of
Award ID300785. The author acknowledges Debbie Whyte
dothiepin in overdose. Lancet 1994; 343: 735.
and Toni Nash for data entry into the Hunter Area ToxicologyService database and Ian Whyte for developing the database.
15 Combes A, Peytavin G, Theron D. Conduction disturbances
associated with venlafaxine. Ann Intern Med 2001; 134:166–7.
16 Khurana RN, Baudendistel TE. Hypertensive crisis associated
with venlafaxine. Am J Med 2003; 115: 676–7.
1 Buckley NA, McManus PR. Fatal toxicity of serotoninergic
17 Chan B, Whyte I, Dawson A, Downes M. Use of neostigmine
and other antidepressant drugs: analysis of United Kingdom
for the management of drug induced ileus in severe
mortality data. BMJ 2002; 325: 1332–3.
poisonings. J Med Toxicol 2005; 1: 18–22.
2 Whyte IM, Dawson AH, Buckley NA. Relative toxicity of
18 Banham NDG. Fatal venlafaxine overdose. Med J Aust 1998;
venlafaxine and selective serotonin reuptake inhibitors in
overdose compared to tricyclic antidepressants. QJM 2003;
19 Malik M, Camm AJ. Evaluation of drug-induced QT interval
96: 369–74.
prolongation: implications for drug approval and labelling.
3 Hojer J, Hulting J, Salmonson H. Fatal cardiotoxicity induced
Drug Saf 2001; 24: 323–51.
by venlafaxine overdosage. Clin Toxicol (Phila) 2008; 46:
20 Hunt AC. Accuracy of popular automatic QT interval
algorithms assessed by a ‘gold standard' and comparison
4 Peano C, Leikin JB, Hanashiro PK. Seizures, ventricular
with a novel method: computer simulation study. BMC
tachycardia, and rhabdomyolysis as a result of ingestion of
Cardiovasc Disord 2005; 5: 29.
venlafaxine and lamotrigine. Ann Emerg Med 1997; 30:
21 Isbister GK, Friberg LE, Hackett LP, Duffull SB.
Pharmacokinetics of quetiapine in overdose and the effect
5 Bosse GM, Spiller HA, Collins AM. A fatal case of venlafaxine
of activated charcoal. Clin Pharmacol Ther 2007; 81: 821–7.
overdose. J Med Toxicol 2008; 4: 18–20.
22 Friberg LE, Isbister GK, Hackett LP, Duffull SB. The population
6 Howell C, Wilson AD, Waring WS. Cardiovascular toxicity due
pharmacokinetics of citalopram after deliberate
to venlafaxine poisoning in adults: a review of 235
self-poisoning: a Bayesian approach. J Pharmacokinet
consecutive cases. Br J Clin Pharmacol 2007; 64: 192–7.
Pharmacodyn 2005; 32: 571–605.
Br J Clin Pharmacol
Source: http://curriculum.toxicology.wikispaces.net/file/view/bcp0067-0572.pdf
Malcolm Gooding, now in his 60s, has recently embarked on three new careers – those of property developer, olive farmer, and guesthouse owner. Forget retirement Join this worldwide giving movement – it's worth it. Get some of the highest interest rates around as well as interest in advance Speeds up recovery.
Huerta, Schade, Granell (Eds): Connecting a Digital Europe through Location and Place. Proceedings of the AGILE'2014 International Conference on Geographic Information Science, Castellón, June, 3-6, 2014. ISBN: 978-90-816960-4-3 Analysing spatiotemporal patterns of antibiotics prescriptions Luise Hutka and Lars Bernard Technische Universität Dresden Professorship of Geoinformation Systems



