Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Microsoft word - 10b.balasad_primary_f.docx
Romanian Neurosurgery (2012) XIX 1: 63 – 66 63
Primary tuberculomas of the thoracal spinal cord. Case report
D. Balasa1, A. Tunas1, A. Terzi2, C. Serban4, M. Aschie3
Clinical Emergency County Hospital, Constanta
1Neurosurgery, 2Anestesiology, 3Pathology
4 Euromedic Private Unit, Constanta, Neuroradiology
Abstract
intramedullary tuberculoma. We present
The authors present an unusual case of
the case of un unusual case of
intramedullary tuberculoma in a HIV-
intramedullary tuberculoma in a HIV-
negative patient from the southeast part of
negative patient from the southeast part of
Romania who demonstrated no other signs
Romania who demonstrated no other signs
of tuberculous infection. Clinical exam:
of tuberculous infection and presents no
extreme spastic paraparesis in triple flexion,
sign of involvement of the bony spinal
dorsal pain and bladder and bowel canal.
incontinence. Gd enhanced MRI revealed
ring enhancing lesion with central
Case report
hypointensity, suggesting granulomatous
Presentation: This 20 years old young
pathology. Surgical excision of the peasant male was referred to our
intramedullary lesions was carried out department for evaluation of his
followed by anti-tuberculous chemotherapy
progressivelly (one year and a half) extreme
and Baclofen tablets . !0 days postoperative
spastic paraparesis in triple flexion, dorsal
MRI showed total resolution of the lesion.
pain, bladder and bowel incontinence.
Two years follow up showed progressive
There was no history of tuberculosis and he
resolution of spasticity. Following surgical
was HIV seronegative.
excision, the patient improved significantly
Examination: On examination the pacient
sensitive and modest the motility and acused un severe spastic paraparesis in
spasticity. The management of this rare
triple flexion and the right leg more
lesion is discussed and the literature profoundly affected than the left. Patellar
and achille relexes was increased. Babinsky
Keywords: spinal cord, tuberculosis, sign was positive. Sensory deficit to p
primary tuberculomas
inpick and light touch revealed a T4 level
right, T5 level left. Chest X-Ray films
Intramedullary tuberculomas rest a revealed no abnormalities.
lesion extremelly rare (2 of 100 000 cases of
Dorsal MRI scan including Gd-DTPA
tuberculosis and 2 of 1000 cases of CNS
MRI revealed ring enhancing lesion with
tuberculosis). Lin and McDonnell (11, 12) central hypointensity, suggesting
found only 148 cases of intramedullary
granulomatous pathology from T4 to T5
tuberculomas mentioned in the literature.
Ratliff (15) present one case of primitive

64 D. Balasa et al Primary tuberculomas of the thoracal spinal cord
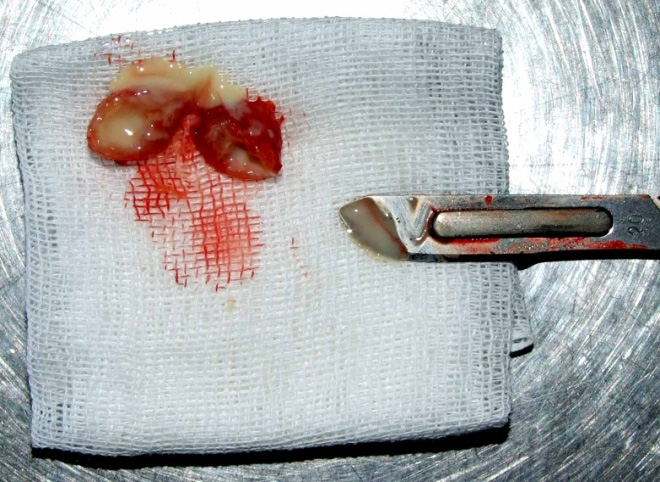
Operation T4-T5 laminectomy, median
mielotomy, microsurgical total resection of
a well circumscribed yellow-grey mass
located cortically and intramedullary. The
lesion was very carefully dissected and
totally resected along a definable plane by
use of the operating microscope.
The gross pathological specimen was an
encapsulated, yellow-grey firm mass.
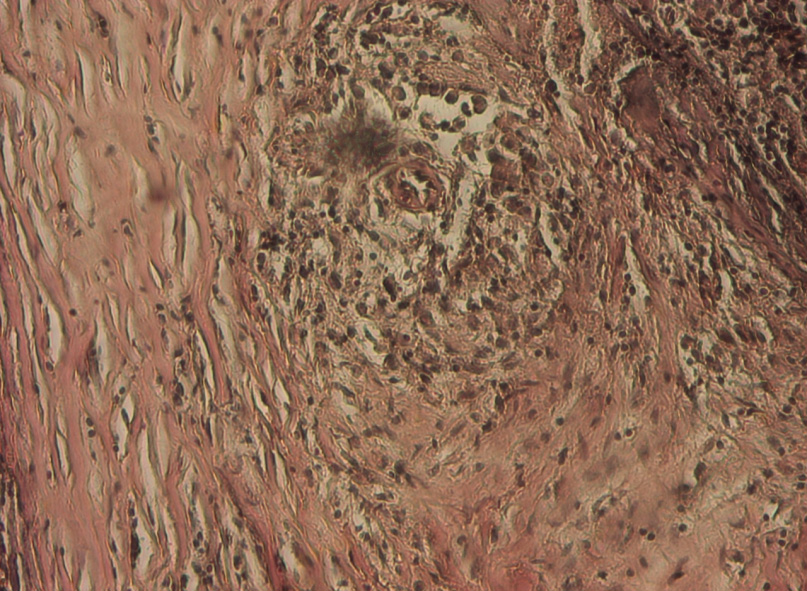
Pathological findings
Ppathological examination of the lesion
revealed multiple epitheloid cell
granulomas with Langerhan's and foreign
body type of giant cells. Large areas of
caseous necrosis were seen and necrotic
Photomicrograph.: Photomicrograph
demonstrating epitelioid areas of caseating
granulomas with Langhans type giant cells.
Van Gieson coloration.
Postoperative course
Medical treatment: antituberculous
chemotherapy for 52 weeks or more consist
of four chemotherapeutic agents to
overcome drug resistance: INH
300mg/day, rifampin 600 mg/day,
etambuthol 1200 mg/day and pyrazinamide
2000 mg/day and antispastic agents
(Baclofen tablets). Ten days postoperative
MRI showed total resolution of the lesion.
The patients improved significantly
sensitivity and modest the motility and
spasticity. Follow up period: 2 years.
Romanian Neurosurgery (2012) XIX 1: 63 – 66 65
cases (11, 12). The first report of
intramedullary tuberculoma was by
Abercrombie in 1828 (1) .The commonest
symptoms were progressive lower limbs
weakness, paresthesia, and bladder and
bowel dysfunction. The major physical
findings were paraplegia, either spastic or
flaccid. The majority of patients had
thoracic sensory level.
The MRI characteristics have been
described by Jena et al (10) as low intensity
rings with or without central hyperintensity
on T2 images and low to isointense rings
on T1 images. Caseation results in the
"target sign" appearance.
The choice of treatment is an important
consideration. Microsurgical total excision
and antituberculous agents are widely used
in the treatment of intramedullary
tuberculoma. MacDonnel has reported 65%
recovery after surgical treatment.
Conclusion
•Intramedullary tuberculoma, is a very
•Microsurgical total excission and
antituberculous chemotherapy consisting of
three agents was mandatory for the healing
this very large intramedullary lesion.
•Motor recovery of this patient is
Discussion
difficult considering the extreme spastic
Tuberculosis is a chronic bacterial paraparesis in triple flexion and the
infection produced by Mycobacterium evolution of the illness of one and a half
tuberculosis Tuberculosis of the central
nervous system is a rare entity, affecting
•Will be necessary in time orthopedic
0,5-2% of patients with sistemic procedures for the treatment of spasticity
tuberculosis (14, 3, 15). Intramedullary
tuberculomas is a lesion extremelly rare
seen only 2 of 100 000 cases of tubeculosis
Corespondence address
and 2 of 1000 cases of tuberculosis of
Dr. D. Balasa, Department Neurosurgery,
central nervous systems disesase. It is Clinical Emergency County Hospital, Boulevard
speciffically for the young patients in the
Tomis, 145, Constanta, Romania. E-mail:
developing countries and is associated [email protected]
usually with pulmonay disease, in 69% of
66 D. Balasa et al Primary tuberculomas of the thoracal spinal cord
References
9. Gupta VK, Jena A,Sharma A,Guha DK, Khushu S, Gupta AK: Magnetic resonance imaging of intracranial
1. Abercrombie J. Pathological and practical researches
tuberculomas. J Comput Assist Tomogr 12:280-285,
on disease of the brain and the spinal cord. Edinburg:
Waugh and Innes, 1828: 371-2
10. Jena A, Banerji AK,TripathiRI, Gulati PK, Jain RK,
2. Alex H.MacDonel, Robert W.Baird, Michael
Khushu S, Supra MI. Demonstration of intramedullary
S.Bronze. Intramedullary tuberculomas of the spinal
tuberculosis By MRI- A case report of 2 cases. Br J
cord:Case report and review. Review of infectious
Radiol 64:555-557, 1991
diseases. Vol 12,3:432-436,1990
11. Lin TH:İntramedullary tuberculoma of the spinal
3. Baker RD: Postmortem Examination. Specific
cord . J Neurosurg 17:497-499, 1960
Methods and Procedures. Philadelphia, W.B. Saunders,
12. MacDonell AH, Baird RW, Bronze MS:Intra Baird
RW, Bronze MS: Intramedullary tubercullomas of the
4. B. Indira Devi, S. Chandra, S. Mongia,
spinal cord: Case report and review. Rev Infect Dis
Chandramouli, K.V.R. Sastry, S. K. Shankar. Spinal
12:432-439, 1990
Intramedullary Tuberculoma and Abscess: A Rare
13. Mohit AA, Santiago P, Rostomily R. Intramedullary
Cause of Paraparesis. Neurology India, Vol 50, No 4,
tuberculoma mimicking primary CNS
Dec 2002, 494-496
Parmar H, Shah J, Patkar D, Varma
5. Bertrand I, Guillaume JM, Samson M, Gueguen Y:
R.Intramedullary tuberculomas. Mr findings in sevens.
Tuberculoma Intamedullarire dorsal. Rev Neurol
patients. Acta Radiol 41:572-7, 2000
15. Ratliff JK: Intramedullary tuberculoma of spinal
6. Citow JS, Ammirati M : Intramedullary tuberculoma
cord. J Neurosurg(Spine) 1999:90:125-128
of the spinal cord. Case report. Neurosurgery 1994; 35:
16. Whiteman M, Espinosa L, Post MDJ, Bell MD,
Falcon S: Central nervous system tuberculosis in HİV
7. Dastur HM. Diagnosis and neurosurgical treatment
infection patient. Clinical and radiographical finding.
of tuberculous disease of the CNS. Neurosurg Review.
AJNR Am J Neuroradiol 16:1319-1327, 1995
1983, 6: 111-117 8. GokalpHZ, Ozkal E: Intradural tuberculomas of the spinal cord. J Neurosurg 1985, 55:289
Source: http://www.roneurosurgery.eu/atdoc/10b.BalasaD_Primary_f.pdf
Blood Eosinophils to Direct Corticosteroid Treatment of Exacerbations of Chronic Obstructive Pulmonary DiseaseA Randomized Placebo-Controlled Trial Mona Bafadhel1, Susan McKenna1, Sarah Terry1, Vijay Mistry1, Mitesh Pancholi1, Per Venge2,David A. Lomas3, Michael R. Barer1, Sebastian L. Johnston4, Ian D. Pavord1, and Christopher E. Brightling1 1Institute for Lung Health, University of Leicester, Leicester, United Kingdom; 2Department of Medical Sciences, Clinical Chemistry, University ofUppsala, Uppsala, Sweden; 3Cambridge Institute for Medical Research, University of Cambridge, Cambridge, United Kingdom; and 4Department ofRespiratory Medicine, National Heart and Lung Institute, Centre for Respiratory Infections, Imperial College London, London, United Kingdom
ciencia y educación ecológica en Chiloé Palabras editoriales: Durante mita compartir responsabi- ¡arte!, forman parte de las esta fría y lidades en el cuidado de los actividades que estamos lluviosa pri- ecosistemas regionales, la realizando y de las que les biodiversidad, los recursos invitamos a informarse en naturales y la comprensión el presente boletín.



