Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Untitled
Dental Traumatology 2009; 25: 541–544; doi: 10.1111/j.1600-9657.2009.00811.x
Management of a complicated crown-rootfracture using adhesive fragment reattachmentand orthodontic extrusionCASE REPORT
Ce´lia Tomiko Matida Hamata Saito,
Abstract – Dental trauma is more common in young patients and its sequelae
Marcos Heidy Guskuma, Je´ssica
may impair the establishment and accomplishment of an adequate treatment
Lemos Gulinelli, Celso Koogi
plan. This paper reports a case of complicated crown-root fracture in a young
Sonoda, Idelmo Rangel Garcia-
adult that was treated using adhesive tooth fragment reattachment and
´ nior, Osvaldo Magro Filho,
orthodontic root extrusion. Considering the time elapsed to follow up, the
Soˆnia Regina Panzarini
fracture extension, the amount of remaining root portion and the patient's low
Department of Surgery and Integrated Clinics,
socioeconomic status, the treatment approach proposed for this case provided
Dental School Arac¸atuba, Sa˜o Paulo State
good functional and aesthetic outcomes. Clinical and radiographic results after
University (UNESP), Arac¸atuba, SP, Brazil
2 years were successful. This case report demonstrates the importance ofestablishing a multidisciplinary approach for a successful dental traumamanagement.
Correspondence to: Profa. Dra. SoˆniaRegina Panzarini, Departamento deCirurgia e Clı´nica Integrada, Disciplina deClı´nica Integrada, Faculdade deOdontologia do Campus de Arac¸atuba,UNESP, Rua Jose´ Bonifa´cio 1193, CEP:1601-050, Arac¸atuba, SP, BrasilTel.: +55-18-3620-3240 or+55-18-3622-5693Fax: +55 18 36363332e-mail:
[email protected]
Accepted on 17 April, 2009
Dental trauma is a more common event in young patients
and its sequelae may impair the establishment andaccomplishment of an adequate treatment plan. Each
A 21-year-old female victim of motorcycle accident was
trauma case should be evaluated on an individual basis (1).
referred to the Oral and Maxillofacial Traumatology and
Crown-root fractures correspond to a significant part
Surgery Service of the Dental School of Arac¸atuba
of cases of tooth injuries and are more prevalent in the
(UNESP, Brazil) after receiving first-aid medical care.
11–18-year-old age group (2). Depending on the exis-
The patient presented with abrasions in the region of the
tence or not of pulp involvement, they may be classified
nose and chin, soft-tissue laceration in the upper lip and
respectively as complicated, which are more frequent, or
a complicated crown-root fracture with pulp exposure in
non-complicated crown-root fractures (2, 3).
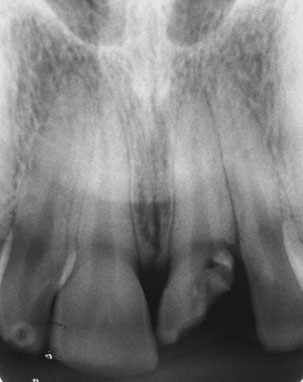
the maxillary left central incisor (Fig. 1). Part of the
There are several treatment strategies for aesthetic and
coronal fragment was in place, attached to the gingival.
functional rehabilitation in cases of crown-root fracture,
The incisal coronal fragment, which was the largest
including mucogingival flap and adhesive reattachment
portion, was found at the site of accident right after the
of the original fragment (4), orthodontic extrusion
first-aid care and was maintained in saline storage until
followed by reconstruction of tooth crown with a
the following treatment session (Fig. 2). Periapical
restorative material (5), orthodontic extrusion followed
radiographs taken from different angulations revealed
by prosthetic rehabilitation (6), adhesive fragment reat-
an oblique root fracture that extended approximately
tachment associated to laminate veneer (7) and inten-
2 mm intraosseous in the distal aspect. The maxillary left
tional replantation (8). Indication of the type of
lateral incisor presented enamel cracks and the neigh-
treatment to be used depends primarily on the bone
bouring teeth presented absence of clinical and radio-
level of fracture.
graphic findings (Fig. 3).
This paper reports a case of complicated crown-root
The emergency dental care aimed to alleviate the pain
fracture in a young adult treated using adhesive tooth
and discomfort. The coronal fragment was gently removed
fragment reattachment and orthodontic extrusion.
under local anaesthesia, the soft-tissue laceration was
Ó 2009 John Wiley & Sons A/S




Saito et al.
treated conservatively with local antiseptic solution, thecoronal pulp was curetted, and the pulp chamberreceived a dressing with a commercially prepared anti-biotic–corticosteroid product (OtosporinÒ, Farmoquı´mi-ca S/A, Rio de Janeiro, RJ, Brazil) and was provisionallysealed with a glass ionomer cement (Vidrion R, SSWhite, Rio de Janeiro, RJ, Brazil). Antibiotic therapy(amoxicillin 500 mg, three times/day; Eurofarma, Sa˜oPaulo, SP, Brazil) was started and maintained for 7 days.
An anti-inflammatory (Potassium diclofenac 50 mgevery 8 h for 3 days; Novartis Biocieˆncias SA, Sa˜oPaulo, SP, Brazil) and an analgesic (Paracetamol 750 mgevery 6 h in case of pain; Aventis Pharma Ltd, Suzano,SP, Brazil) were also prescribed.
Two days after the emergency visit, an exploratory
Fig. 1. Pre-operative clinical view.
surgery showed that the fracture complicated crown-rootextended deeply subgingivally, invading the biologicalwidth in the distal aspect and reaching 2 mm below thebone crest (Fig. 4). In the same session, the coronalfragment maintained in saline storage was reattached tothe root remnant using and adhesive restorative techniquewith a total-etch adhesive system (Single Bond; 3M/ESPE,St Paul, MN, USA) and a light-cured microhybridcomposite resin (TPH, Dentsply Ind. e Com. Ltda,Petro´polis, RJ, Brazil). The restoration of the fracturedcrown was completed with composite resin (Fig. 5). Dueto the loss of tooth structure, a bevel was made on theremaining root portion to increase fragment retention.
An adequate adaptation of the incisal fragment to the
Fig. 2. Incisal coronal fragment.
Fig. 4. Clinical aspect during the exploratory surgery showingthe extension of the complicated crow-root fracture, invadingthe biological width in the distal aspect.
Fig. 5. Clinical aspect after adhesive coronal fragment reat-
Fig. 3. Pre-operative periapical radiograph.
Ó 2009 John Wiley & Sons A/S


Crown-root fracture and orthodontic extrusion
Fig. 8. Clinical view after 24 months of follow up.
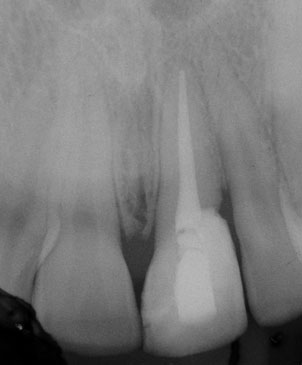
Fig. 6. Periapical radiograph after adhesive coronal fragmentreattachment.
Fig. 9. Radiographic aspect after 24 months of follow up.
Fig. 7. Fixed appliance used for orthodontic extrusion installed
right central incisor and maxillary left lateral incisor, at
and activated.
the incisal third, to provide the necessary anchorage fortooth movement (Fig. 7). A 0.012-inch stainless steelwire (Dental Morelli) was bent to form a 2-mm diameter
distal aspect of the apical fragment was not possible due to
loop with a 4-mm radicular extension, which was further
the invasion of the biological width (Fig. 6). Endodontic
roughened with diamond disks to provide retention and
therapy started with removal of pulp tissue from the
was cemented with glass ionomer cement (Vidrion R, SS
remaining root portion under copious 1% sodium
White) in the coronal root canal third of the fractured
hypochlorite irrigation (Milton solution, Asfer-Industria
tooth. Next, a 1/8 diameter orthodontic elastic was
Quimica Ltda, Sa˜o Caetano do Sul, SP, Brazil), instru-
placed through the coronal loop and tied to the palatal
mentation and placement of a calcium hydroxide-based
bow fixed between the neighbouring teeth. The elastic
intracanal dressing for 30 days. Definitive root canal
string was changed once a week. Orthodontic extrusion
obturation was performed thereafter with lateral conden-
was terminated when all root margins were exposed,
sation of gutta-percha points (Tanari; Tanariman Indus-
which was achieved within 21 days. After reestablish-
trial Ltda., Manacapuru, AM, Brazil) and Sealapex root
ment of the biological width, the tooth was splinted with
canal sealer (Kerr Corp., Orange, CA, USA), leaving the
composite resin (TPH, Dentsply) for 12 weeks and a
coronal third unfilled.
mucoperiostal flap repositioning surgery was performed
Orthodontic extrusion was performed using a fixed
in the area surrounding the extruded tooth. The
appliance to re-establish the biological width. A 0.028-
treatment was completed with post space preparation
inch round stainless steel orthodontic wire (Dental
and cementation of a metallic radicular post (FKG
Morelli, Sorocaba, SP, Brazil) was fixed with light-cured
Dentaire, La-Cheaux-de Fonds, Switzerland) to provide
composite resin to the palatal surface of the maxillary
resistance to the fractured tooth. The palatal access was
Ó 2009 John Wiley & Sons A/S
Saito et al.
sealed with composite resin and tooth/composite sur-
patient's age, the treatment proposed for this case,
faces were repaired with composite resin, polished and
combining adhesive tooth fragment reattachment and
adjusted for occlusal interferences.
orthodontic root extrusion, provided good functional
Clinical and radiographic follow up after 24 months
and aesthetic outcomes. Clinical and radiographic results
showed a good adaptation of the tooth fragment/
after 2 years were successful. This case report demon-
composite resin restoration, absence of radiographic
strates the importance of establishing a multidisciplinary
signs of root resorption and absence of painful symp-
approach for a successful management of dental trauma.
tomatology (Figs 8 and 9).
1. Canoglu H, Gungor HC, Cehreli ZC. Management of cervical
One of the determinant factors for the functional and
root fracture using orthodontic extrusion and crown reattach-
aesthetic success in the management of complicated
ment: a case report. Oral Surg Oral Med Oral Pathol Oral
crown-root fractures is the adoption of a multidisciplin-
Radiol Endod 2007;104:46–9.
2. Castro JCM, Poi WR, Manfrin TM, Zina LG. Analysis of the
ary approach involving surgery, endodontics, periodon-
crown fractures and crown-root fractures due to dental trauma
tics and prosthodontics (6) The literature shows that
assisted by the Integrated Clinic from 1992 to 2002. Dent
coronal restoration of teeth with crown-root fracture is
usually challenging, especially when the fracture extends
3. Andreasen FM. Reattachment of subgingivally fractured cen-
below the bone level (9), as occurred in the present case.
tral incisor with an open apex. Dent Traumatol 2007;23:263–4.
Different treatment strategies have been proposed for
4. Eden E, Yanar SC, So¨nmez S. Reattachment of subgingivally
cases of complicated crown-root fracture including
fractured central incisor with an open apex. Dent Traumatol
surgical exposure of the fractured surface, orthodontic
5. Emerich-Poplatek K, Sawicki L, Bodal M, Adamowicz-Klep-
or surgical extrusion of the apical fragment, intentional
alska B. Forced eruption after crown/root fracture with a
replantation and tooth extraction in more severe cases
simple and aesthetic method using the fractured crown. Dent
(1, 4–8, 10, 11).
Orthodontic extrusion was the treatment of choice to
6. Poi WR, de Cardoso L, de Castro JC, Cintra LT, Gulinelli JL,
re-establish the biological width in this case because it is
de Lazari JA. Multidisciplinary treatment approach for crown
considered a safe procedure with respect to the occur-
fracture and crown-root fracture – a case report. Dent
rence of root resorption and does not involve loss of
periodontal support or bone tissue of the surrounding
7. Nandlal B, Daneswari V. Restoring biological width in crown-
root fracture: a periodontal concern. J Indian Soc Pedod Prev
teeth, which favours aesthetics (12–14).
Although adhesive fragment reattachment cannot be
8. Wang Z, Heffernan M, Vann WF Jr. Management of a
considered a durable procedure for the management of
complicated crown-root fracture in a young permanent incisor
extensive fractures (5), this technique offers an effective
using intentional replantation. Dent Traumatol 2000;24:100–3.
and conservative treatment option in some cases because
9. Koyuturk AE, Malkoc S. Orthodontic extrusion of subgingi-
this technique shortens the operative time and improves
vally fractured incisor before restoration. A case report: 3-years
the reproduction of tooth colour, shape and contour (15).
follow-up. Dent Traumatol 2005;21:174–8.
On the other hand, the reconstruction of a fractured
10. Heda CB, Heda AA, Kulkarni SS. A multi-disciplinary
tooth with composite resin is a good alternative for
approach in the management of a traumatized tooth withcomplicated crown-root fracture: A case report. J Indian Soc
young patients, having the advantage of preserving the
Pedod Prev Dent 2006;24:197–200.
remaining root portion and providing an immediate
11. Villat C, Machtou P, Naulin-Ifi C. Multidisciplinary approach
resolution to the case, which is particularly important for
to the immediate esthetic repair and long-term treatment of an
patients that cannot afford a prosthetic rehabilitation
oblique crown-root fracture. Dent Traumatol 2004;20:56–60.
(16). In the present case, composite resin reconstruction
12. Bach N, Baylard JF, Voyer R. Orthodontic extrusion: peri-
was associated with tooth fragment reattachment. The
odontal considerations and applications. J Can Dent Assoc
reduced resistance of the restored tooth to the mastica-
tory efforts was compensated by the cementation of an
13. Benenati FW, Simon JHS. Orthodontic root extrusion: its
rationale and uses. Gent Dent 1986;34:285–9.
intracanal retainer. Although the use of the tooth
14. Heithersay GS. Combined endodontic-orthodontic treatment
fragment reattachment technique is not common in these
of transverse root fractures in the region of the alveolar crest.
cases, it is important that dentists warn their patients on
Oral Surg Oral Med Oral Pathol 1973;36:404–15.
the importance of collecting fragments of teeth fractured
15. Cengiz SB, Kocadereli I, Gungor HC, Altay N. Adhesive
due to traumatic injuries and instruct them on the use of
fragment reattachment after orthodontic extrusion: a case
adequate wet storage medium, so that the fragments can
report. Dent Traumatol 2005;21:60–4.
be suitable for reattachment (4).
16. Panduric V, Gabric D, Negovetic-Mandic V. Immediate post-
Considering the time elapsed to follow up, the fracture
traumatic upper incisor reconstruction using composite resinmaterials. Dent Traumatol 2008;24:108–11.
extension, the amount of remaining root portion and
Ó 2009 John Wiley & Sons A/S
Source: http://www.maxillofacialcenter.com.br/artigos/fratura_corono-radicular_complicada.pdf
DISCOVER • DEVELOP • DELIVER Medical innovation that helps millions of patients around the world EBE is a specialised group of European Federation of Pharmaceutical Industries and Associations, EFPIA ContentP4 • Introduction P5 • Value of Biopharma P5 • What role does biotechnology play in healthcare? P6 • How biopharmaceutical and small-molecule medicines differ
LYMPHATIC FILARIASIS MORBIDITY PROJECT SURGICAL HANDBOOK An Aid to District Hospital Surgeons 2nd edition, Summer 2007 LF -Filaricele surgery handbook* IMPORTANT NOTICE: Techniques described in this Handbookare only for treating LF patients who have normal scrotal skin! Surgical techniques described here and during The West Africa LF-Morbidity Project's training workshops are contraindicated inpatients with significant lymphoedema of the scrotal skin,elephantiasis of the scrotum, or lymph-scrotum. Such conditionsmay generally require reconstructive surgery.



