Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Jrgodontologia.com.br

Autologous fat grafts placed around temporomandibular joint
total joint prostheses to prevent heterotopic bone formation
Larry M. Wolford, DMD, Carlos A. Morales-Ryan, DDS, MSD, Patricia Garcia Morales, DDS, MS,
and Daniel Serra Cassano, DDS
the treatment of ankylosis
This study evaluated 1) the efficacy of packing autologous fat grafts
of the temporomandibular
around temporomandibular joint (TMJ) total joint prosthetic reconstruc-
joint (TMJ) was reported
tions to prevent fibrosis and heterotopic bone formation and 2) the ef-
by Blair (2) in 1913 and
fects on postsurgical joint mobility and jaw function. One hundred fifteen
by Murphy (3) in 1914. In
patients (5 males and 110 females) underwent TMJ reconstruction with
1992, Thomas (4) reported
total joint prostheses and simultaneous fat grafts (88 bilateral and 27
the use of autologous fat
unilateral) for a total of 203 joints. The abdominal fat grafts were packed
transplantation to prevent
around the articulating portion of the joint prostheses after the fossa
heterotopic bone forma-
and mandibular components were stabilized. Patients were divided into
tion after hip replacement
two groups: group 1 (n = 76 joints) received Christensen total joint
surgery in six patients. In
prostheses, and group 2 (n = 127 joints) received TMJ Concepts total
orthopedics, radiation of
joint prostheses. Clinical and radiographic assessments were performed
the operated area is gener-
before surgery, immediately after surgery, and at long-term follow-up. In
ally used to prevent het-
group 1, maximal incisal opening (MIO) increased 3.5 mm, lateral excur-
erotopic bone formation
sions (LE) decreased 0.2 mm, and jaw function improved 1.9 levels. In
group 2, MIO increased 6.8 mm, LE decreased 1.4 mm, and jaw function
The problem of het-
improved 2.4 levels. The improvement for MIO and patient perception of
erotopic calcification is
jaw function in both groups was statistical y significant; no significant dif-
frequently seen after place-
ference was found for LE. There was no radiographic or clinical evidence
ment of alloplastic materi-
Figure 1. A coronal tomogram of a
of heterotopic calcifications or limitation of mobility secondary to fibrosis
als in the TMJ, particularly prosthetical y reconstructed TMJ joint
demonstrates heterotopic bone forma-
in either group. Twenty-five Christensen prostheses (33%) were removed
when al oplasts of Proplast/
tion (arrows) between the mandibular
because of device failure and/or metal hypersensitivity; no fibrosis or het-
Teflon (Vitek Inc., Hous-
ramus and medial side of the fossa. No
erotopic bone formation was seen at surgical removal. Four TMJ Concepts
ton, TX) or Silastic (Dow-
fat graft was placed around the prosthe-
prostheses (3%) were removed because of metal hypersensitivity. In all
Corning, Midland, MO)
sis at surgery.
instances, removal of the prostheses was unrelated to the autologous
have been previously im-
fat grafting. Ten patients (8.7%) developed complications involving the
planted (8) (Figure 1). Heterotopic bone can also result from
fat donor site: two patients (1.8%) developed abdominal cysts requiring
trauma, reactive arthritis, osteoarthritis, sepsis, inflammation,
surgery, and eight patients (6.9%) developed seroma formation requiring
and connective tissue/autoimmune diseases such as rheuma-
aspiration. Autologous fat transplantation is a useful adjunct to prosthetic
toid arthritis, psoriatic arthritis, ankylosing spondylitis, and
TMJ reconstruction to minimize the occurrence of excessive joint fibrosis
scleroderma. These calcifications can cause continued worsening
and heterotopic calcification, consequently providing improved range of
pain and a progressive decrease in range of motion that may
motion and jaw function.
lead to bony ankylosis. A variable amount of fibrosis and possibly
The first report of autologous fat transplantation appeared From the Department of Oral and Maxilofacial Surgery, Texas A&M University
in the literature in 1893 (1). Since then, autologous fat
Health Science Center Baylor College of Dentistry and Baylor University Medical Center, Dal as, Texas (Wolford; Morales-Ryan and Cassano were former fel-
grafting has been used extensively in humans for vari-
lows); private practice, Laredo, Texas (Morales-Ryan, Garcia Morales); and the
ous applications. Among these are aesthetic procedures
Department of Pediatric Dentistry, Araraquara Dental School, São Paulo State
for contour augmentation, particularly in the maxillofacial re-
University, Brazil (Cassano).
gion, and ablative procedures, as in the treatment of various
Corresponding author: Larry M. Wolford, DMD, 3409 Worth Street, Suite 400,
injuries of the frontal sinus. The use of autologous fat grafts in
Dallas, Texas 75246 (e-mail: [email protected]).
Proc (Bayl Univ Med Cent) 2008;21(3):248–254

reactive tissue are commonly as-
significant differ-
sociated with the heterotopic
ence was noted in
bone, thereby worsening the ef-
the patients' percep-
fect. Pharmacologic treatment
tion of their pain
cannot predictably prevent the
level at long-term
development of these unwanted
follow-up. There
tissues in the TMJ. Durr and Tur-
was no radiographic
lington (9) have reported favor-
or clinical evidence
able outcomes in two thirds of
of heterotopic cal-
their patients with TMJ ankylosis
cifications or limi-
by using postsurgical radiation.
tation of mobility
However, significant concerns
secondary to fibro-
exist about the effects of this
sis in any of the fat-
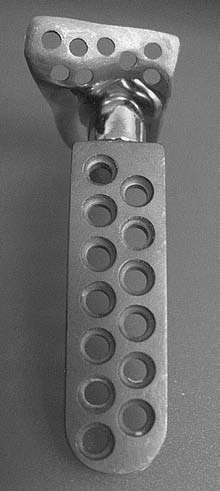
Figure 3. The TMJ Concepts total joint prosthesis
treatment on nearby structures
grafted group, while
is a patient-fitted device, constructed on a three-
(e.g., brain, orbit, parotid gland).
7 control patients dimensional model and designed for each patient's
Additional y, the TMJ region is
specific anatomical requirements. The devices
more vascular than the hip, and
heterotopic bone
have metal-on-polyethylene articulations.
the frequent presence of particu-
and required reop-
lated polymeric materials may
eration. This initial study proved that autologous fat transplan-
preclude a successful result with
Figure 2. The Christensen pros-
tation was a useful adjunct to prosthetic TMJ reconstruction.
radiation. Other surgeons' expe-
thesis is an off-the-shelf device
The technique minimizes the occurrence of excessive joint fi-
riences with radiation therapy
with three selections for the man-
brosis and heterotopic calcification and consequently provides
in patients with recurrent TMJ
dibular component and over 40
improved range of motion. No other published studies in the
selections for the fossa compo-
ankylosis have not been favor-
literature involve the placement of fat grafts around total joint
nent. The best-fitting components
able (personal communication,
are selected to fit the anatomy.
Dr. Robert V. Walker, Dallas,
These devices have metal-on-
This study evaluates the treatment outcomes after TMJ re-
TX, and Dr. Stephen S. Fennell,
construction with total joint prostheses and fat grafts in a much
Athens, GA).
larger group of patients.
In 1992 Wolford developed the philosophy and technique
for placing fat grafts around TMJ total joint prostheses to pre-
PATIENTS AND METHODS
vent heterotopic bone formation, decrease fibrosis, improve
Inclusion criteria for this study were as follows: 1) patients
pain levels, and increase jaw function. Wolford and Karras (10)
had unilateral or bilateral TMJ reconstruction using total joint
published the first study evaluating fat grafts placed around TMJ
prostheses with abdominal fat grafts packed around the pros-
total joint prostheses. Fifteen patients (2 males and 13 females)
theses' area of articulation; 2) all patients were operated on by
underwent TMJ reconstruction with Techmedica (Techmedica,
one surgeon (LMW) at Baylor University Medical Center in
Inc., Camarillo, CA) custom-made total joint prostheses (cur-
Dal as, Texas; 3) adequate records were available for analysis; and
rently manufactured by TMJ Concepts Inc., Ventura, CA).
4) the minimum fol ow-up was 1 year. Records of 115 consecu-
Surgery was bilateral in 7 patients and unilateral in 8, for a total
tive patients (5 males and 110 females) meeting these criteria
of 22 joints. All patients had autologous fat harvested from
were evaluated; 88 patients had bilateral and 27 had unilateral
the abdomen grafted around the articulating portion of the
TMJ reconstruction, for a total of 203 joints. The patients were
joint prostheses after the fossa and mandibular components had divided into two groups. Group 1 (n = 42; 76 joints) received
been stabilized. Twenty patients (2 males and 18 females) who
Christensen total joint prostheses (TMJ Implants Inc., Golden,
received Techmedica total joint prostheses without fat grafts
CO) (Figure 2), and group 2 (n = 73; 127 joints) received TMJ
served as a control. There were 17 bilateral and 3 unilateral Concepts total joint prostheses (TMJ Concepts Inc., Ventura,
cases, for a total of 37 joints.
CA) (Figure 3).
In the fat graft group, average maximum incisal opening
For all patients, total joint prostheses were placed and sta-
(MIO) was 26.9 mm preoperatively and 38.7 mm at long-
bilized, and then autologous fat harvested from the abdomen
term fol ow-up, an improvement of 11.8 mm. Contralateral
was packed around the articulating portion of the prostheses.
excursive movements (LE) averaged 2.3 mm preoperatively and Clinical and radiographic assessments were performed before
2.2 mm at long-term follow-up. In the non–fat-grafted group,
surgery (T1), immediately after surgery (T2), and at longest
the average MIO was 26.8 mm preoperatively and 33.1 mm at
follow-up (T3). Objective clinical evaluations of MIO and LE
long-term fol ow-up, an improvement of 6.3 mm. Contralateral
were determined from T1 and T3 data, whereas jaw function
excursive movements averaged 3.2 mm preoperatively and 1.7
was subjectively evaluated according to a numerical analog
mm at long-term follow-up. The differences in measured func-
scale (0 = normal jaw function and 10 = no jaw function).
tion between the two groups were statistically significant (P ≤
Student's t test was used to determine statistical significance at
0.01). Although both groups experienced a decrease in pain, no the P ≤ 0.01 level. Radiographic evaluation compared T2 and
Autologous fat grafts placed around temporomandibular joint total joint prostheses to prevent heterotopic bone formation
the fat a variable dis-
tance depending on
the fat pad thickness
and the amount of
graft required (usual
range per joint, 5–20
cc). The fat was then
widely undermined
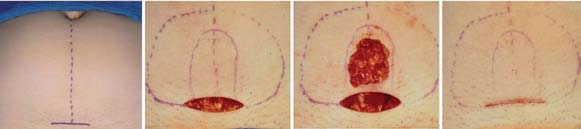
Figure 4. Fat graft harvesting technique used in this study. (a) The fat graft is harvested from the abdomen, usual y through a 4- to 5-cm incision general y made in the suprapubic area. (b) The outer dashed line is the extent of undermining of the skin and beneath the fat pad.
superficial to the rec-
The inner solid line denotes the fat graft to be harvested. (c) The abdominal fat graft harvesting is complete. (d) 3-0 polyglactin sutures
tus abdominis muscle
are used to close the deep fat layers so no depression in the harvest area wil be evident. The skin is closed with subcuticular suturing.
fascia to a similar ex-
tent as the overlying
skin dissection. The desired amount of graft was harvested in
a single block from the midline region (Figure 4c). To allow
for shrinkage and errors in estimation, this amount was 20%
to 30% more than the estimated amount needed to fill the
dead space in the TMJ region. Meticulous hemostasis was
achieved with electrocautery, and the defect in the fat pad was
closed by advancing the lateral fat flaps toward the midline and
suturing with 3-0 polyglactin. The skin incision was closed
with subcutaneous sutures of 4-0 polydioxanone (Figure 4d),
and adhesive skin closures were placed for reinforcement. To
minimize the incidence of hematoma and seroma formation,
a pressure dressing of fluffed gauze and elastic tape was applied
and maintained for approximately 3 days before removal.
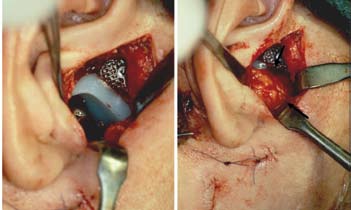
Figure 5. Surgical technique used in this study. (a) The fossa component prosthesis is placed through an endaural or preauricular incision. The mandibular component
The graft was immediately placed through the endaural or
is placed through a submandibular incision. (b) The abdominal fat graft (arrows) is
preauricular incision to fill the dead space around the articulat-
packed into the joint space to prevent heterotopic bone formation and fibrosis.
ing portion of the prosthetic components (Figure 5). In bilateral
cases, the graft was divided into equal portions, and one portion
T3 x-rays (panographic x-rays, linear tomograms, and lateral
was stored in iced normal saline until placement in the second
cephalograms) for the presence of postsurgical heterotopic bone
side. The fat was packed into the TMJ region relatively firmly,
formation around the prostheses. Donor site complications without causing excessive tissue damage to the graft. The wound
were also evaluated.
was closed in routine layered fashion.
Surgical technique
The prostheses were placed through endaural or preauricular
The average patient follow-up period was 31.2 months
and submandibular incisions, as previously described (8), after
(range, 12–65 months). The study results are summarized in
thorough debridement of the region. Fol owing stabilization of
the Table. Both groups had a statistically significant improve-
al condylar and fossa components, fat was harvested from the
ment in MIO and patient perception of jaw function at long-
abdomen. The abdomen was prepared and draped in routine fash-
est fol ow-up, but the improvement was greater for group 2.
ion from above the umbilicus to the pubic region. The superior
Neither group had a significant difference in LE. There was no
portion of the pubic hair was shaved,
if necessary, to place the incision as
low as possible on the abdomen for
Table. Objective and subjective clinical data for 115 patients before and ≥1 year after
optimal cosmesis. If an existing scar
temporomandibular joint total joint prosthetic reconstructions with autologous fat grafts
was present in the lower abdomen,
this site was used instead.
A 4- to 5-cm transverse incision
was made in the midline through
1: Christensen total joint
skin and subcutaneous tissue to ex-
prostheses (n = 76 joints)
pose the abdominal fat pad (Figure
2: TMJ Concepts total joint
4a, 4b). The skin was widely under-
prostheses (n = 127 joints)
mined superiorly and lateral y, tak-
*Assessed through a numerical analog score: 0 = normal function; 10 = no function.
ing care to maintain a 3- to 5-mm
†P ≤ 0.01 for T3 vs T1.
layer of fat on the skin side. The ini-
MIO indicates maximum incisal opening; LE, maximum lateral excursion; T1, before surgery; T3, at long-term fol ow-up.
tial incision was then deepened into
Baylor University Medical Center Proceedings
Volume 21, Number 3


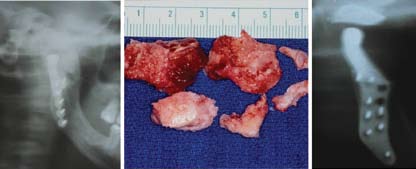
Figure 7. Case 1. (a, b, c) Presurgery, the patient had a class I occlusion on the left side and a class I occlusion on the right side. (d, e, f) The occlusion remained stable 2 years after surgery.
Figure 6. Case 1. (a, b) This 45-year-old man was referred after 14 previous failed right TMJ surgeries; the most recent involved right TMJ reconstruction with a total joint prosthesis (Osteomed system)
without a fat graft. He had severe TMJ and myofascial pain, head-aches, and difficulty eating. (c, d) The patient 2 years after right Figure 8. Case 1. (a) The presurgical panographic x-ray showed massive heterotopic bone TMJ debridement, removal of heterotopic bone and the Osteomed formation (outlined by arrows) around the Osteomed prosthesis. (b) The heterotopic bone prosthesis, TMJ reconstruction with a TMJ Concepts patient-fitted was removed in sections. (c) A 10-year postsurgical radiograph shows the effectiveness of total joint prosthesis, and fat grafting.
the fat graft in preventing heterotopic bone development.
radiographic evidence of heterotopic bone formation in either
these eight patients required drain placement postsurgery for
group at longest follow-up.
evacuation of persistent seroma formation.
Of the 76 Christensen prostheses, 25 (33%) were removed
because of elevated pain levels due to device failure (fracture CASE PRESENTATIONS
or loosening of the fossa component) or metal hypersensitivity
caused by metallosis from the metal-on-metal articulation. No
This 45-year-old man (Figure 6a, 6b) was referred to the
fibrosis or heterotopic bone formation around the prostheses
senior author after undergoing 14 previous failed right TMJ
was observed at surgical removal. The removed Christensen
surgeries, including procedures using devices that contained
prostheses were replaced with TMJ Concepts total joint pros-
Proplast/Teflon. He was 2 years post–TMJ reconstruction with
theses and simultaneous fat grafting around the articulating an Osteomed total joint prosthesis (Osteomed Inc., Dallas,
area of the prostheses. Of the 127 TMJ Concepts prostheses, 4 TX) without the placement of a fat graft around it at that
(3%) were removed from two patients because of severe metal
surgery. He had severe TMJ and myofascial pain, headaches,
hypersensitivity: one patient was sensitive to molybdenum and
and difficulty eating. He presented with a class I occlusion
one to nickel. The latter patient developed dense fibrous tissue
on the left side and a class II occlusion on the right side (Fig-
around the prostheses, but no bone. The other patient main-
ure 7a–c). There was massive heterotopic bone development
tained the fat grafts around her prostheses. The prostheses in
and bony ankylosis surrounding the right TMJ (Figure 8a),
these patients were replaced with TMJ Concepts prostheses that a foreign body giant cell reaction secondary to the previous
had ion-treated titanium condylar heads, eliminating the cobalt-
Proplast/Teflon materials, and a severely limited incisal open-
chromium-molybdenum alloy head that also contained 1%
ing of 20 mm with no translation of the right condyle.
nickel. Fat grafts were again placed around the prostheses.
The TMJ reconstructive surgery was performed in one op-
The fat donor sites were evaluated, and 10 patients (8.7%)
eration and included 1) unilateral right TMJ debridement and
developed complications: two extremely obese patients (1.2%)
removal of heterotopic bone formation around the old prosthesis
developed abdominal cysts superficial to the rectus abdominis (Figure 8b); 2) removal of the Osteomed prosthesis; 3) unilateral
muscle that required surgical removal; eight patients (6.9%)
right TMJ reconstruction with patient-fitted TMJ Concepts total
developed seroma formation requiring aspiration, and two of
joint prosthesis (Figure 5a); and 4) packing of autologous fat
Autologous fat grafts placed around temporomandibular joint total joint prostheses to prevent heterotopic bone formationitle here
attempts at surgical correction by rib grafting had
failed. He had only 3 mm of incisal opening and was
developing significant dental problems because of his
inability to receive dental care; he also had severe facial
asymmetry as wel as sleep apnea symptoms. A 3-D
computed tomography scan demonstrates the magni-
tude of the ankylosis (Figure 10a). A TMJ Concepts
total joint prosthesis was manufactured to reconstruct
the TMJ as well as advance and vertically lengthen the
right mandibular ramus (Figure 11a). He underwent
the following procedures in one stage: 1) right TMJ
Figure 9. Case 2. (a) This 12-year-old boy had right TMJ ankylosis, and two attempts at
removal of a large mass of heterotopic bone (Figure
correction by rib grafting (without fat grafts) had failed. With only 3 mm of incisal opening,
10b); 2) reconstruction of the TMJ and mandibular
he was developing significant dental problems, marked facial asymmetry, and sleep apnea. (b, c) The patient 2 years after right-side TMJ reconstruction and mandibular advancement
advancement with TMJ Concepts total joint prosthesis
with a TMJ Concepts total joint prosthesis and fat graft. He had improved facial balance and
(Figure 11a); and 3) fat graft packed around the pros-
good jaw function (35-mm opening) without pain.
thesis and area of previous heterotopic bone formation
to prevent bone from redeveloping. The patient was
evaluated 2 years postsurgery and showed improved
facial balance and good jaw function (35-mm opening)
without pain (Figure 9b, 9c). At the 2-year evaluation,
there was no radiographic evidence of heterotopic bone
formation (Figure 11b).
The formation of extensive fibrosis and hetero-
topic bone has been problematic after total joint re-
Figure 10. Case 2. (a) A 3-D computed tomography scan demonstrates the magnitude of the
construction of the TMJ, as well as from other types
heterotopic bone and joint ankylosis. (b) The heterotopic bone was removed in sections.
of TMJ arthrotomies (Figures 1, 8a, 10a). This is
particularly true of multiply operated joints and joints
with previously failed alloplastic implants. These complica-
tions have been reported to occur after both prosthetic and
autologous joint reconstructions (11). Fibrosis is related to
scar tissue deposition, especially in multiply operated joints,
with a persistent inflammatory response possibly contributing
in joints with previously failed alloplasts. Heterotopic bone
may be deposited in a similar reaction after al oplastic implant
failure. Additional y, the presence of dead space after extensive
joint debridement leads to hematoma formation in this area,
with subsequent organization. Pluripotent cells may then be
induced to differentiate into fibroblasts and osteoblasts, with
Figure 11. Case 2. (a) A TMJ Concepts total joint prosthesis was custom made
deposition of collagen and bone, respectively. In excessively
to reconstruct the TMJ and advance and vertically lengthen the right mandibular ramus. A fat graft was packed around the prosthesis to prevent heterotopic bone
fibrotic joints, there is a decrease in vascularity and thereby
from redeveloping. (b) The tomogram shows no heterotopic bone formation
a decrease in oxygen tension in the surrounding tissues that
around the prosthesis 2 years after surgery.
can lead to the transformation of fibrous tissue into cartilage
graft around the right TMJ prosthesis (Figure 5b). At 2 years
In the orthopedic experience, various pharmacologic agents,
postsurgery, the patient showed good stability (Figure 6c, 6d) with
most notably indomethacin and etidronate, have been used
elimination of TMJ pain, headaches, and myofascial pain and im-
with varying success (13, 14). Pharmacologic therapy has been
proved jaw function. The occlusion remained stable (Figure 7d–f).
suggested for use after prosthetic TMJ reconstruction, but no
At 10 years postsurgery, his incisal opening was 42 mm with 2
substantial data exist regarding its effectiveness (8). In the senior
to 3 mm of translation of the right condyle and no radiographic
author's (LMW's) experience with these medications, the results
evidence of heterotopic bone formation (Figure 8c).
have been very disappointing.
Radiation treatment of the operated area within 4 days
of prosthetic hip reconstruction is now common practice to
This 12-year-old boy developed right TMJ ankylosis at the
control heterotopic bone formation in orthopedic procedures.
age of 1 year secondary to sepsis (Figure 9a). Two previous
However, local radiation of the TMJ raises concerns regarding
Baylor University Medical Center Proceedings
Volume 21, Number 3
potential adverse effects on adjacent vital structures (i.e., eye and
peritoneal perfo-
associated structures, brain, middle ear, and parotid gland), and rations, or post-
it may be ineffective due to the substantially greater vascularity
surgical ileus. In
of the maxil ofacial region. However, Durr et al (9) reported on
our first several
10 patients (15 TMJs) with bony ankylosis surgically managed
with either costochondral grafts, gap arthroplasty, or debride-
serted a suction
ment of heterotopic bone and treated early postoperatively with drain and left it
radiation, 10 Gy in five fractions. With a mean follow-up of
19 months, 10 of 15 TMJs did not show heterotopic bone
development. The only complication identified was parotitis
in three patients (30%).
The rationale for placing autologous fat grafts is to obliter-
Figure 12. Histological examination of a fat graft
ate the dead space present around the joint prosthesis, thus
However, with biopsy taken 4 years after implantation around a
preventing the formation and subsequent organization of a careful attention
TMJ Concepts total joint prosthesis shows viable
hematoma. Creating this physical barrier serves to minimize
fat stil present without evidence of inflammation,
the presence of pluripotent cells and prevents the formation
heterotopic bone formation, or significant fibrosis.
of extensive fibrosis and heterotopic calcification. It may also
at surgery is rarely
isolate any residual reactive tissue from previous alloplastic
needed. Placing a fluffed gauze dressing and securing with elas-
failure to the periphery of the region, minimizing its formation
tic tape or, alternatively, placing a Velcro-secured abdominal
around the joint components. The net result, as evidenced by binder minimizes the incidence of this complication.
the data collected, is a decrease in and perhaps elimination of
Autologous fat grafting appears to be a useful adjunct to
the incidence of heterotopic bone formation and an improve-
prosthetic reconstruction of the TMJ and may prove to be
ment in jaw function.
similarly beneficial in autologous reconstruction. Graft pro-
The ultimate fate of the transplanted fat is unknown. Stud-
curement is quick and easy, with minimal morbidity.
ies of fat transplantation to other anatomic areas show a vari-
able amount of resorption, with a decrease in volume ranging
from 20% to 75% (15, 16). As an adjunct to prosthetic joint
The results of this study demonstrate the efficacy of TMJ
reconstruction, the ultimate resorption of a portion of the
reconstruction with total joint prostheses and simultaneous
graft may not be detrimental to the result. If the formation
autologous fat grafts to the articulating area of the joint. A sta-
of the initial hematoma, fibrosis, and reactive tissue can be
tistical y significant improvement in MIO and patient percep-
prevented, the incidence of complications may be reduced.
tion of jaw function occurred in both groups. The removal of
We have had an occasional opportunity to clinically and his-
25 Christensen prostheses and 4 TMJ Concepts prostheses was
tologically evaluate fat-grafted TMJ Concepts joints postsur-
due to complications associated with prosthesis failure or metal
gery (Figure 12). Clinically, the fat grafts appeared viable, hypersensitivity, but was not fat graft related. No evidence of
with some samples with strands of collagen present but no
fibrosis or heterotopic bone formation was radiographically
evidence of an inflammatory process. The consistency of the
or clinical y observed. The most common complication found
tissue around the prosthesis was significantly softer than that
in the donor area was seroma, which was usually easily treated
seen in the non–fat-grafted patients. Histologically, viable fat
with aspiration and a pressure dressing.
was observed (Figure 12).
The technique of graft procurement is straightforward,
with minimal potential for complications. In our surgeries,
1. Neuber H. Fettransplantation. Chir Kong Verhandl 1893;1:66.
the senior author harvests the fat grafts just prior to graft
2. Blair VP. Operative treatment of ankylosis of the mandible. Trans South
placement, requiring only about 15 minutes of additional
Surg Assoc 1913;28:435.
3. Murphy JB. Arthroplasty for intra-articular bony and fibrous ankylosis of
surgical time. However, some surgeons may prefer to have
the temporomandibular articulation. JAMA 1914;62:1783.
two surgical teams working concurrently so the operation is
4. Thomas BJ. Heterotopic bone formation after total hip arthroplasty. Orthop
not prolonged. Harvesting the fat grafts prior to beginning
Clin North Am 1992;23(2):347–358.
the TMJ reconstruction is not recommended, as this would
5. Fingeroth RJ, Ahmed AQ. Single dose 6 Gy prophylaxis for heterotopic os-
require the grafts to be "on the table" for an extended time,
sification after total hip arthroplasty. Clin Orthop Relat Res 1995;317:131–
likely resulting in significant loss of graft viability. In bilateral
6. DeFlitch CJ, Stryker JA. Postoperative hip irradiation in preven-
cases, it usually takes at least 4 hours to prepare the TMJs
tion of heterotopic ossification: causes of treatment failure. Radiology
and place the prostheses before the fat grafts can be placed.
Therefore, procuring the fat graft just before placement will
7. Maloney WJ, Jasty M, Willett C, Mulroy RD Jr, Harris WH. Prophylaxis
maximize graft viability.
for heterotopic bone formation after total hip arthroplasty using low-dose
Possible complications of abdominal fat graft harvesting
radiation in high-risk patients. Clin Orthop Relat Res 1992;280:230–234.
8. Wolford LM, Cottrell DA, Henry CH. Temporomandibular joint recon-
include hematoma, seroma, infection, ileus, and inadvertent
struction of the complex patient with the Techmedica custom-made total
peritoneal perforation. To date, we have had no infections,
joint prosthesis. J Oral Maxillofac Surg 1994;52(1):2–10.
Autologous fat grafts placed around temporomandibular joint total joint prostheses to prevent heterotopic bone formation
9. Durr ED, Turlington EG, Foote RL. Radiation treatment of heterotopic
13. Francis MD, Russell RG, Fleisch H. Diphosphonates inhibit formation
bone formation in the temporomandibular joint articulation. Int J Radiat
of calcium phosphate crystals in vitro and pathological calcification in
Oncol Biol Phys 1993;27(4):863–869.
10. Wolford LM, Karras SC. Autologous fat transplantation around temporo-
14. Ritter MA, Gioe TJ. The effect of indomethacin on para-articular ec-
mandibular joint total joint prostheses: preliminary treatment outcomes.
topic ossification following total hip arthroplasty. Clin Orthop Relat Res
J Oral Maxillofac Surg 1997;55(3):245–251.
11. MacIntosh RB. Costochondral and dermal grafts in temporomandibular
15. Carpaneda CA, Ribeiro MT. Study of the histologic alterations and vi-
joint reconstruction. Oral Maxillofac Surg Clin North Am 1989;1:363–
ability of the adipose graft in humans. Aesthetic Plast Surg 1993;17(1):43–
12. Hall BK. Cartilage: Biomedical Aspects, vol. 3. New York: Academic Press,
16. Hörl HW, Fel er AM, Biemer E. Technique for liposuction fat reimplanta-
tion and long-term volume evaluation by magnetic resonance imaging.
Ann Plast Surg 1991;26(3):248–258.
Baylor University Medical Center Proceedings
Volume 21, Number 3
Source: http://jrgodontologia.com.br/blog/wp-content/uploads/2011/11/Autologous-Fat-Graft1.pdf
¿Qué es lo que pretenden los estudiantes chilenos? Para una nueva educación Página 8 época V - N° 168 emPadronamiento debe decirnos cómo estamos, no quiénes somos Censo y educación 2/ La Paz, septiembre de 2012 La Paz septiembre de 2012 / REFLEXIÓN PEDAGÓGICA "La educación es el arma más poderosa que tú puedes
Miniature Books for Sale Catalog 54: March 1, 2015 KAREN NYMAN 702 Rosecrans Street San Diego CA 92106-3013 All books are in very good or better condition unless otherwise noted. Shipping within the USA is $3 whether you buy one book or more. If you are overseas, I will have to look into the costs for mailing to your country. To see a photo of any book, please ask and I will scan an image of the cover to you in an email. Books are shipped to you on approval; they are returnable for any reason within one week of purchase. Please pay promptly after you have received your books with a check payable to Karen Nyman and mail to address above. Overseas buyers may pay with PayPal but it is necessary to contact me first.



