Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Doi:10.1016/j.jep.2007.05.009

Journal of Ethnopharmacology 113 (2007) 100–110
Medicinal perceptions of vegetables traditionally consumed
by South-Asian migrants living in Bradford, Northern England
Andrea Pieroni , Laura Houlihan, Nafeesa Ansari, Bushra Hussain, Saiqa Aslam
Division of Pharmacy Practice, School of Life Sciences, University of Bradford, Richmond Building,
Richmond Road, Bradford BD7 1DP, West Yorkshire, UK
Received 22 December 2006; received in revised form 14 March 2007; accepted 1 May 2007
Available online 10 May 2007
Dietary habits change rapidly amongst migrant communities in Western countries, and these changes can cause major concerns for public-health
policymakers because they frequently lead to increases in diet-related diseases like diabetes. Such is the case in most South-Asian communitiesin the UK. In this study, we carried out an ethnobiological survey of the vegetables traditionally consumed among the Indian and Pakistanicommunities of Bradford, in Western Yorkshire, UK. Our purpose was to analyse in depth details of the traditional culinary use of vegetableswithin these households, and to assess the health perceptions of them.
Semi-structured interviews with a total of 150 South-Asian women were carried out. Twenty-five vegetables were recorded, as well as their
traditional culinary use and their frequency of use. We found that a few of these vegetables, particularly those presenting bitter or aromatic tastes,were perceived to have remarkable medicinal value particularly against diabetes. Our study also found important generational differences in thewomen's knowledge of the culinary processes related to these foods, confirming that the consumption of traditional vegetables is inextricablyembedded in cultural heritage and the representation of identity among migrants.
Our findings may offer evidence of a link between the choice of food and the foods' perceived medicinal value among South-Asian migrants.
It may also provide important information for health care professionals when designing strategies for improving health care counteracting type 2diabetes. We strongly believe such strategies should take into account socio-cultural components and emic health beliefs, as well as patients' viewsof traditional dietary ingredients.
2007 Elsevier Ireland Ltd. All rights reserved.
Keywords: Urban ethnobotany; Ethnopharmacy; Trans-cultural pharmacy; South-Asians; Diabetes; Bradford
According to a recent estimate, by 2036 the number of patientsaffected by type 2 diabetes among the overall British popula-
It is generally agreed that South-Asian migrants living in
tion will rise by at least 20% If this is the
Western countries are at high risk of developing type 2 dia-
case, the disease will become one of the NHS's most crucial
challenges, because type 2 diabetes is already four times more
example, have recently exposed a high prevalence of
common among British South-Asians than among the general
diabetes mellitus and related conditions in Asian Indians living
in the United States. Using a community-based survey on more
A possible explanation for this phenomenon is related to
than one thousand Asian-Indian migrants living in and around
the metabolic impact of the westernised diet (environmental
the metropolitan area of Atlanta, Georgia, they found an overall
hypothesis) (on South-
prevalence of diabetes mellitus of 18.3%, which is much higher
Asians, and consequently to the cultural change and adaptation
than in Whites, Blacks and Hispanics living in the United States.
in the dietary habits that this group has had to face after dis-placement and migration.
Other studies have underlined that the level of physical activ-
ity among South-Asians is lower than in the general population,
∗ Corresponding author.
and that may also contribute to their increased risk of diabetes
E-mail address: (A. Pieroni).
0378-8741/$ – see front matter 2007 Elsevier Ireland Ltd. All rights reserved.
doi:
A. Pieroni et al. / Journal of Ethnopharmacology 113 (2007) 100–110
On the other hand, several scholars have emphasised that
of traditional food ingredients and various different dishes could
the high prevalence of type 2 diabetes among all ethnic groups
enable general practitioners and other health-care professionals
(including Europeans) could be related to relative poverty, inac-
to provide better care and advice to the Pakistani migrants living
tivity and obesity (and suggest that the
in UK and in Western countries generally
permanence of distinct social classes may strongly affect pat-
It is well known in the ethnosciences that many plants and
terns of health Nevertheless, the issue
foods have been and continue to be ingested because of their per-
of diabetes among South-Asians is surely a central one for
ceived medicinal and health-benefiting characteristics
public health in the UK, and, at present, public-health poli-
Nevertheless, very little
cies are concentrated on improving the efficacy of prevention
research has been carried out in urban Western societies with the
and the understanding of the socio-cultural backgrounds of this
purpose of analysing the grey area between food and medicine,
phenomenon within ethnic minorities, as well as the ‘internal
and so far almost no research in this area has been conducted
strategies' that these communities put in place to counteract it.
in relation to migration phenomena. Instead, most studies have
On this latter aspect, we would suggest that there could be a
focused on the use of traditional medicines among migrants
strong need for more sensitive socio-medical research.
A recent study (has shown, for example,
food plants uses and migrants' cuisine (
that British Pakistani and British Indian patients in Edinburgh are
making deliberate efforts to reduce their intake of oral hypogly-
on more general ethnobotanical issues
caemic agents (OHAs) without being advised to do so. Reasons
So far there has been only a few studies that have addressed
for this include perceptions that the drugs work by providing
the issue of the perceived overlap between food and medicine
relief of symptoms rather than cures, and concerns that OHAs
among migrants in Europe (
could be detrimental to health if taken for long periods, in con-
junction with other drugs, or without traditional foods, like
even though such knowledge could be crucial to a better under-
curries and chapattis, as these foods are perceived as having
standing of the strategies migrants put in place to maintain their
strengthening and fortifying properties that balance the side-
health, prevent illness, and perhaps even manage chronic dis-
effects of the OHAs.
South-Asians, and in particular the Pakistani community in
Similarly, a better understanding of the health perceptions
Bradford, represent one of the largest migrant communities in
and beliefs related to the consumption of traditional plant-based
the UK. Most of the South-Asian migrant community in Brad-
foods within South-Asian migrant communities could be very
ford originally came from the northern Mirpur area of Pakistan
important in improving the implementation of public-health pro-
in the 1950s and 1960s The 1991 Census indi-
grammes aimed at preventing diabetes and also offering help to
cates that Bradford's South-Asian population numbered about
those migrant households that have members affected by the
65,450, making up 14% of the city's total population. At that
disease. A recent survey has suggested
time Bradford had the second highest concentration of people
that public-health projects should involve ethnic minorities as
of Pakistani origin in Britain. The latest estimates indicate that
active participants in the development of appropriate educational
the South-Asian population has grown considerably over the last
programs and material. Hence, studies aimed at understanding
decade to 94,250 and that this population now represents about
health and dietary practices and beliefs among migrant commu-
19% of the total population of Bradford
nities represent an important starting point for providing timely
studied how food is perceived among
inputs for improving such policies.
second-generation British-Pakistanis in Bradford, and has found
Accordingly, the aims of this study have been:
that while first-generation migrants perceive their own food asbeing traditional and tasty (but problematic for health), they
• to record the culinary use, the frequency of use and the
perceive English food as being foreign and bland (and paradox-
preference for traditional vegetables among the South-Asian
ically more healthy). Jamal also found that younger generations
community of the Bradford area;
of British-Pakistani increasingly consume English foods. Other
• to determine the perception of taste and the (eventual) medic-
studies, however, have pointed out that inter-generational dif-
inal value that migrant women ascribe to these vegetables;
ferences in the diets of first- and second-generation Pakistani
• to briefly discuss eventual implications of this study for
Muslims in Bradford are minimal (Recent
public-health policies and dietary and health counselling
research carried out on Asian migrants in Bradford has shown a
directed specifically at South-Asian migrants in the UK.
rising incidence in childhood diabetes (Problems for the Bangladeshi community in accessing diabetes
2. Methods
services in Bradford have already been well analysed however, other authors have showed that there is huge
Fieldwork was conducted over a period of 10 weeks from
resistance to slimming and healthy diets among these commu-
March to May 2005 in local Asian greengrocers in Brad-
nities (It is therefore essential to fully under-
ford, where first-generation and second-generation Pakistani and
stand the emic perception of health and well-being related to tra-
Indian women customers were approached in the morning hours,
ditional diets and medicines among South-Asians, because accu-
and asked a few questions using a simple questionnaire and brief
rate estimations of their perceptions of the medicinal properties
semi-structured interviews. Most of the participants were elderly
A. Pieroni et al. / Journal of Ethnopharmacology 113 (2007) 100–110
(n = 93/150 over 60 years old), female (n = 140/150), and first-
3. Results
generation (n = 124/150) migrants. Most of the informants wereunable to communicate in fluent English, so all the interviews
all the recorded vegetables, together with the
were carried out in Urdu or Punjabi by the authors NA, BH, and
vernacular names they are known by among migrant commu-
nities in Bradford, their botanical Latin names, the parts of the
Nineteen interviewees agreed to be visited and interviewed
plant that are used in the kitchen, their most common culinary
in more depth at home. In-depth interviews were tape recorded,
preparations – as quoted by at least five informants, and the fre-
and later transcribed and translated into English.
quency of their consumption (based on the average of the quotes
Prior Informed Consent (PIC) was obtained verbally before
given by all the informants). Most of the recorded vegetables are
commencing each interview. Ethical approval was granted by
consumed fresh or cooked with vegetable oil and in the presence
the University of Bradford Ethics Committee. Ethical guidelines
of a variety of different spices. Many of the youngest informants
adopted by the American Anthropological Association (
were unable to describe in detail the culinary processes used for
were rigorously followed.
each named taxa, suggesting that their traditional knowledge of
Questions about the use of various food plants were asked
vegetables is mainly passive.
using classical means of ethnobotanical analysis (
These data show clearly that traditional knowledge (TK)
related to culinary uses of vegetables among South-Asian
migrants is quite sophisticated; for each given vegetable it was
Participants were asked at the beginning of the semi-
possible to trace a specific preferred culinary preparation. Also,
structured interviews to free-list traditional vegetables they use
no significant differences were detected among the culinary
in their daily cuisine. In the context of this study, we have defined
practices of British Pakistani and British Indian women, except
as "traditional" those ingredients that the interviewees knew
for the Indian women's slight preference for pickling fragrant
and/or had been used in their country of origin. For each named
manjack fruits (Cordia dichotoma, Boraginaceae).
item, we asked for exact details of how the food is prepared, its
the most-quoted vegetables. No significant
frequency of use, taste, perceived healthiness, (eventual) medic-
differences were found between the data provided by the British
inal properties, and the (eventual) presence of food taboos. In
Pakistani and the British Indian women. Similarly, no quali-
determining the vegetables' perceived healthiness, we used the
tative differences regarding the kind of quoted vegetables were
following scale, which the main author (AP) had already devel-
found among different generations of interviewed women. Bitter
oped in a previous ethnobiological study
melon (karela, Momordica charantia) and okra (bhindi, Hibis-cus esculentus) represented the most cited vegetables by nearly
• 1: no recognised health value;
the half of the interviewees. The prevalence of these two veg-
• 2: middle-low health value ("that food is healthy");
etables is not surprising since their culinary use is very popular
• 3: middle-high health value ("that food is very healthy");
and widespread throughout the South-Asian sub-continent
• 4: high health value ("that food is almost like a medicine");
• 5: very high health value ("that food is a medicine!").
the perceived taste and the medicinal prop-
erties of the selected vegetables. Most of the quoted plants have
We deliberately avoided asking specifically and directly
been defined as having either a "soft, bland or a sweet" taste,
about "medicinal foods", in order to limit bias.
while only five vegetables were perceived as having a "bitter"
One hundred and fifty women informants were interviewed
taste. Two vegetables were described as having an "aniseed-like
in total, 55% (n = 82/150) of whom were Indian and 45%
taste". This perception was categorized with a unique cogni-
(n = 68/150) were Pakistani. Each named plant item was col-
lected, photographed, identified, dried, and deposited at the
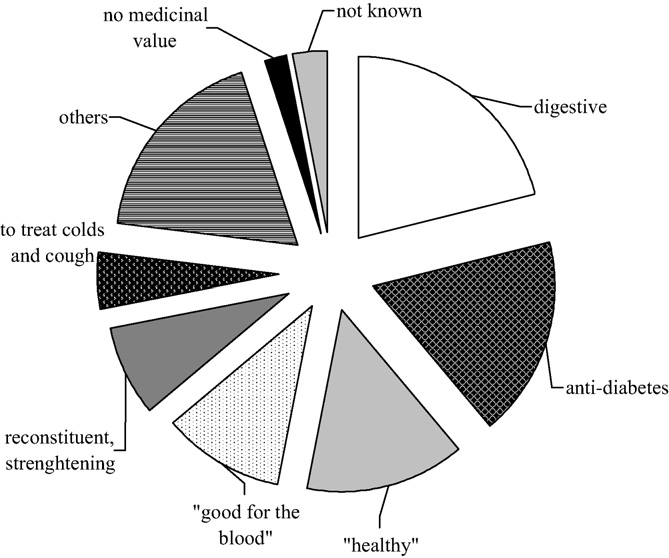
ws the different medicinal properties attributed to
Herbarium of the Laboratory of Pharmacognosy at the Univer-
the quoted vegetables. Most of the plants are thought to have
sity of Bradford (PSGB). Botanical nomenclature followed the
anti-diabetic properties or to aid digestion. A discrete portion of
rules of Mansfeld's World Database of Agricultural and Horti-
the vegetables is simply considered to be "healthy", or good for
strengthening the body, or suitable as a tonic. Others are reputed
Some of the informants quoted spices; these data were how-
to be "good for the blood". The frequent citation of presumed
ever not analysed, as the focus of the research was to investigate
anti-diabetic properties of a few vegetables (especially bitter
vegetables; moreover, the perceived medicinal properties of
melon) suggests that South-Asian women are well aware of the
many traditional spices used in the cuisine of the South-Asian
health problems in their households, and perhaps adopt their
sub-continent are already very well known in both ethnobotany
own strategies for preventing or counteracting diabetes. These
strategies may be very different from those followed by West-
When recording the participants' perceptions of the medic-
ern bio-medical schools, or even by the South-Asian traditional
inal properties of the vegetables, the original emic descriptions
practitioners, who are also widespread in the area.
and definitions were retained in order to avoid translating them
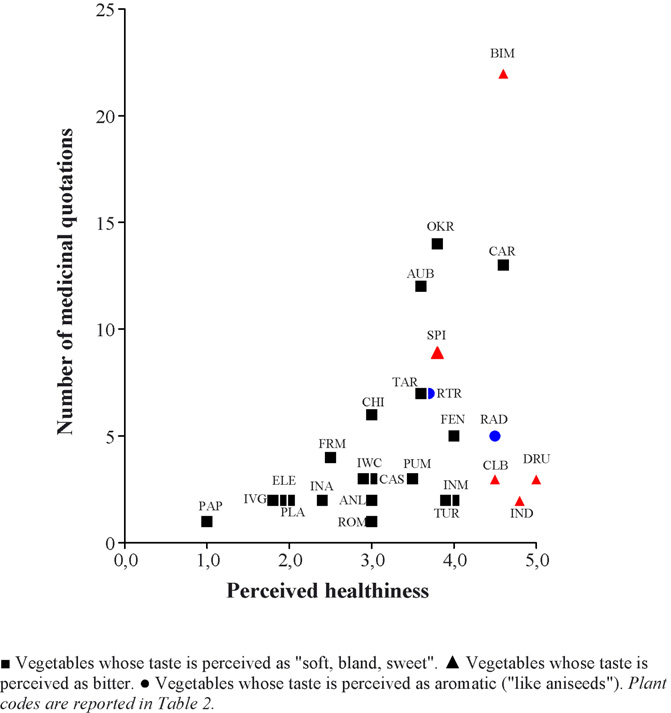
the correspondence among the recorded per-
into bio-medical Western concepts. Information regarding the
ceived healthiness, the number of medicinal claims, and the
main issues addressed during the interviews was analysed and
perceived taste of the recorded South-Asian vegetables. As can
elaborated using ANTHROPAC (
be seen, vegetables perceived as bitter are mostly considered
Table 1Traditional vegetables consumed by South-Asian migrants in Bradford
Botanical name and family
Traditional culinary preparation(s)
Anethum sowa Roxb. ex
The aerial parts are chopped and added to spinach and fenugreek
leaves, fried garlic, chillies and turmeric
The roots can be peeled and eaten raw, or they can be washed and
Willd. (Liliaceae)
peeled, cut into strips and placed in an airtight container along withwashed lemons and limes, sliced carrots, salt, cumin. The mixtureis then covered with mustard oil, and stored for at least a monthbefore eating
Brassica juncea (L.) Czern.
Sarson ka sag (sag)
The leaves are chopped, and then boiled in water with green chillies
for a few hours. At the end of the cooking time, chopped ginger and
garlic, previously fried in oil, are added together with fresh
Brassica rapa L. var. rapa
Onion, garlic and ginger are fried in sunflower oil, spices are added
and then the meat. Once the meat is tender, the peeled and chopped
turnips are added. The mixture is then cooked on low heat
Carica papaya L.
The fruit is cut in half and the seeds are removed, then it is cooked
in oil for one hour with onions and spices
Cicer arietinum L.
The fresh chickpeas are removed from the pods and fried with
onions, garlic and spices. Water can be added to make a soup, or the
peas can be eaten with chapattis. They can also be eaten withpotatoes or meat, or added to salads after being boiled. Entirechickpea pods can be fried or roasted in the oven
Coccinea grandis (L.)
The fruit is peeled and chopped, and fried in oil with garlic and
Voigt (Cucurbitaceae)
ginger paste, and sometimes tomatoes and spices. The mixture isoften served with yoghurt
Colocasia esculenta (L).
The leaves are washed and left to dry, then chickpeas paste is spread
Schott. (Araceae)
on the leaves and they are rolled up, sliced, and deep fried in oil
Colocasia esculenta (L).
The arvi is peeled, washed and diced, and fried in oil along with
Schott. (Araceae)
onions and garlic, various spices, and/or other vegetables or meat.
They can also be peeled and sliced and deep-fried as chips
Cordia dichotoma G. Forst.
Lasooras are cut in half, the seeds are removed, and the fruit is
washed to remove the stickiness. Then they are boiled and pickledin oil with spices. They are stored in jars with whole chillies andgreen lemon/lime segments
Cucurbita maxima Duch.
The kadoo is peeled, chopped into little pieces and fried with
ex Lam. (Cucurbitaceae)
onions, garlic and spices. Lentils that have been previously beenboiled can also be added
The beans are chopped and cooked with onions and garlic in oil.
(L.) Taub. (Fabaceae)
Often tomatoes and turmeric or sugar and peas are added. Theselegumes are generally served with boiled rice
Daucus carota L.
Peeled and chopped, carrots are fried alone or with onions, garlic
and spices. These can be added to other vegetables, or potatoes, ormeat. Alternatively, the carrots can be boiled in water with salt andpepper. They can also be ground and cooked for over 4–5 h withplenty of milk and sugar to make a dessert. After thickening, themixture is placed in the fridge to cool
Hibiscus esculentus L.
Once the tops are chopped off, the fruit is cooked in oil or ghee
with garlic, onions, ginger and turmeric. It can also be added tomeat dishes once the meat is tender. Lemon juice is often squeezedon bhindi to prevent them sticking together. At other times thesevegetables are simply boiled in salted water and eaten, or they canbe split in half and filled with gram flour, crushed peanuts andonions, and gently cooked in oil
Luffa acutangula (L.)
The fruit is stuffed with raw onions, garlic, ginger, chillies, and
Roxb. (Cucurbitaceae)
coriander, and then gently fried in oil, with more onions andtomatoes. It can be also diced into small pieces and saut´eed withchopped onions, and flavoured with garlic, ginger and turmericwith small pieces of chopped potatoes added
Momordica charantia L.
The vegetable is peeled and then cut in half lengthwise, and the
internal parts are scooped out. These are mixed with spices and salt,and the two halves are put back together, tied with string and gently
fried with onions in oil. The fruit can be also split in half and filled
with gram flour, peanuts, crushed onions, garlic, and sometimes
sugar (to sweeten the karela). It is then cooked slowly. The bitter
melon can also chopped up into a pulp, a pinch of salt is added, and
the liquid is given to diabetic patients to drink
Moringa oleifera Lam.
Once washed, the outer husk is peeled off and the fruit is fried with
onions, ginger, turmeric, chillies and often, tomatoes andaubergines. This fruit is often served with yoghurt. Sometimes the
entire fruit is used, and their outer layers are spat out
Musa paradisiaca L.
The fruit is peeled, sliced and boiled, and once it is soft enough, it
is fried in oil with various spices
If eaten with meat, first onions are fried in oil along with spices,
(Stocks) Pang.
ginger and garlic, and then the meat is added. Once the meat is
cooked, the sliced melon is added. If used by itself, the melon issliced, gently fried in oil and spices, and often served with yoghurt
Raphanus caudatus L.
Rat-tailed radish
Mougri is chopped and cooked in oil with onions and spices. It is
generally eaten with meat but it can also be chopped up and eaten
raw with yoghurt and cucumber
Raphanus sativus L.
These can be peeled and eaten raw or added to salads. They can
also be grated, left for half an hour to remove excess water, then
added to finely chopped onions, green chillies, salt and coriander.
The mixture is then cooked in butter and used to stuff chapattis.
Radishes can also be pickled. First they are cut in large chunks,green chillies and salt are added, and the mixture is covered withvinegar and left to sit for 1–2 h. Radish pickles can be eaten thesame day
Solanum melongena L.
The aubergine is washed, the top is removed and the rest is chopped
into little pieces. It is then fried in oil or butter with tomatoes,onions and sometimes garlic. Spices are also added. Sometimes thechopped aubergine is cooked with potatoes or peas. It is oftenserved with squeezed lemon juice, or sliced in half lengthwise andfilled with flour and crushed onions, then fried in oil with variousspices
Spinacia oleracea L.
The leaves are chopped, and then fried in sunflower or corn oil,
together with garlic, onions and spices (generally turmeric, gingerand chillies). Often potatoes or peas, or chicken or lamb pieces arealso added
A. Pieroni et al. / Journal of Ethnopharmacology 113 (2007) 100–110
Most quoted traditional vegetables consumed in South-Asian households
"healthy", even if they are not necessarily the most quoted ones
(the exception being bitter melon).
4.1. Traditional vegetables in the South-Asian migrant diet
In this study, we recorded twenty-five vegetables that were
quoted by South-Asian women. Among the more uncommon
recorded food items we listed were drumstick (Moringa oleifera,
Moringaceae), fragrant manjack (Cordia dichotoma, Boragi-naceae), rat-tailed radish (Raphanus caudatus, Brassicaceae),and Indian asparagus (Asparagus racemosus, Liliaceae s.l.).
Most of the recorded vegetables are still very frequently con-
sumed in South-Asian migrant households.
The majority of the quoted vegetables were perceived to
have medicinal properties It is interest-ing to underline, however, that more than half of the perceivedmedicinal properties of the quoted vegetables refer to specificpathologies. In other words they represent real food-medicines ormedicinal foods. Moreover, most of the quoted vegetables were
perceived as folk functional foods (
Fig. 1. Perceived (emic) medicinal character of the recorded traditional South-
Asian vegetables.
A. Pieroni et al. / Journal of Ethnopharmacology 113 (2007) 100–110
Table 3Perception of taste, healthiness and medicinal properties of the recorded vegetables
Perceived medicinal properties (and number of informantsclaiming them)
Treats diabetes (2)
Soft, sweet, bland
"Strengthens the body" (6); Garam ("it makes you warm whenyou are feeling cold inside") (2); good for general health (2);"helps the mind" (1); "good for the joints" (1)
Very bitter, hot, spicy and tangy
Treats diabetes (19); heals constipation (1); good for generalhealth (1); provides vitamins (1)
"Good for the eyes" (9); prevents diabetes (1); "good for theblood" (1); "good for the brain" (1); good for general health (1)
Strengthening food ("good if you are feeling low") (2); preventsdiabetes (1)
Prevents the flu (3); good for general health (2); "good for thejoints" (1)
Treats diabetes (2); anti-arthritic (1)
Slightly bitter
Treats diabetes (1); anti-arthritic (1); relieves back pains (1)
Good for general health (2)
Leafy, with a slightly bitter taste
Good for general health (7); Garam ("It makes you warm whenyou are feeling cold inside") (1)
Treats coughs and colds (4)
Digestive, good source of iron (2)
Indian water chestnut
Bitter, potatoe-like texture
Treat back pains in the elderly (1); Digestive (1); "Good forpregnant women" (1)
Soft, tangy, bland
Heals constipation (5); reconstituent (4); strengthen joints (2);anti-arthritic (1); good for general health (1); digestive (1)
"It has contraceptive properties; should be avoided by womenof child bearing age" (1)
Bland, sometime sweet
Good for general health (2)
Good for general health (1); "helps stomach acid" (1);"liquefies fat" (1)
Watery, aniseed-like
Prevents diabetes (4); diuretic (1)
Rat-tailed radish
Hot, aniseed-like
Digestive (4); to treat diabetes (2); anti-arthritis (1)
Good for general health (1)
"Strong", slightly bitter
Strengthening food (4); good for general health (2); treatsconstipation (1); "provides vitamins" (1); "good for the blood"(1)
Sweet, soft, slippery
Good for general health (3); treats constipations (2); relievesstomach-aches (1), "good for the joints" and for treatingarthritis (1)
"Good for blood flow" (1); anti-cholesterolemic (1)
In italics are marked taste perceptions that refer to bitter taste.
and many of the women told us that "all vegetables are good for
of diagnostic tests carried out by the usual health primary care
actors (GPs and hospitals). Nevertheless, most of interviewed
Ethnoscientific studies carried out during the last decade have
migrants felt that they needed to also adopt their own healing
pointed out the inextricable connection between food and eth-
strategies to be used in conjunction with allopathic medications
nomedical practices (
prescribed by their GPs. Most of the women interviewed seemed
to believe that the "healing" properties ascribed to specific plant
has been confirmed in our study, and we strongly feel that besides
foods could also have a more general, preventive effect on other
their taste, the perceived medicinal value of vegetables is also
(apparently healthy) family members.
crucial in their appreciation.
While carrots, cassava and radish are thought to prevent
diabetes, angular loofah (Luffa acutangola), cluster beans
4.2. Traditional strategies to manage diabetes
(Cyamopsis tetranogloba), drumsticks, rat-tailed radish, andespecially bitter melon were quoted by the South-Asians women
Our informants were clearly very concerned about the preva-
as botanicals that are able to be used to "treat" diabetes.
lence of diabetes among their family members and neighbours.
The ascribed anti-diabetic properties of bitter melon in par-
In the mind of our informants diabetes was often associated with
ticular are well known in the medical ethnography of the
obesity; however, cases of it were always confirmed as a result
South-Asian subcontinent and
A. Pieroni et al. / Journal of Ethnopharmacology 113 (2007) 100–110
4.4. Consumption of traditional vegetables andgenerational differences
Ethnic food traditions tend to be one of the cultural traits
that pose the most resistance to change in terms of modernisa-tion and adaptation to the host country. From our interviews,we found that older South-Asian migrants tend to prefer a typ-ically Asian diet, whereas younger migrants tend to adapt tothe British way of life more quickly. During the interviews, theelderly informants were able to immediately identify traditionalmethods of preparing the vegetables, which unfortunately thesecond generation migrants were unfamiliar with. One elderlyIndian informant described how bitter melon was cut up andthe inside scooped out, pulped, and then simply drunk withsalt in order "to treat diabetes". In this case the frequencyof consumption apparently depends on the individual's per-ceived level of need for diabetic control (individuals assessthis need after regular blood tests they had carried out withinthe NHS structures, generally after periodic visits to their localGP).
Another interesting concept that was explained during
the interviews was the classification of garam. Fenugreek
Fig. 2. Correspondence among perceived healthiness, number of medicinal
(Trigonella foenum–graecum) and aubergine (Solanum melon-
claims, and perceived taste of the recorded South-Asian vegetables: (�) vegeta-
gena) were both described as having garam properties. The
bles whose taste is perceived as "soft, bland, sweet"; (�) vegetables whose taste
concept of garam originates from the humoral concept that
is perceived as bitter; (䊉) vegetables whose taste is perceived as aromatic ("like
poor health results from a lack of equilibrium between ‘hot'
aniseeds"). Plant codes are reported in
and ‘cold', hence a cold food will be used to treat a hot illness.
One informant explained how aubergine could be used to exert a
many bio-scientific studies conducted during the last decade
‘garam effect' on joint pain in arthritis. Indians classify rheuma-
have confirmed them (
toid conditions as being a cold, windy illness caused by cold,
windy food, cold and windy weather, and cold activities. Theytherefore believe these conditions should be treated with warmfood.
4.3. Does the taste matter?
4.5. Dynamics and changes of traditional diets among
Studies of emic perception of taste in ethnobotany have shown
South-Asians in Bradford
that taste is culturally determined, and can strongly influence theuse and medicinal perception of the plants (
Cooking and consuming traditional vegetables is seen among
In show how the four vegetables consid-
the elderly generations as a central part of cultural heritage,
ered to be bitter are reputed to be very healthy, even when a large
hence traditional vegetables may be a means of strengthening
number of medicinal quotations or a high perceived medicinal
their cultural identity and representing it to the autochthonous
value was not indicated. This could be due to the fact that all bit-
ter vegetables with the exception of Indian dill are considered to
In contrast to the results of other field
be important for counteracting diabetes, hence they have a very
specific "medicinal" perception.
found that the elderly South-Asian migrants in Bradford con-
Informants often explained us that the anti-diabetic proper-
tinue to be conscious of the importance of traditional diet, and
ties of bitter vegetables are due to the fact that "bitter foods
cultural adaptation processes have not yet dramatically changed
counteract the sugars (sweet) in the blood".
the way they feed their families as they may have done in other
It is also evident that the two vegetables that were indicated
areas in Europe.
by the people as having an aromatic taste (radish and rat-tailed
Since ethnicity is also the result of a social process
radish) are among those that were rated most highly for health-
and cultural boundaries are very
dynamic, it would be well worthwhile to follow changes in the
This could suggest that there is a specific role played by
appreciation of traditional vegetables among the South-Asian
taste in the adaptive behaviour of human beings, especially in
migrants of Bradford and elsewhere. On the other hand, we
their cognitive categorisation of "medicinal plants"
cannot forget that cultural boundaries are also partly constructs
created by our own processes of representation
and that food habits are highly
A. Pieroni et al. / Journal of Ethnopharmacology 113 (2007) 100–110
dynamic and therefore able to change very rapidly in response
The women we interviewed free-listed vegetables they gen-
to continuously moving cultural negotiations.
erally process in their households. We suggest that the reasonswhy they quoted these particular few ingredients instead of oth-
4.6. Traditional consumption of South-Asian vegetables:
ers could have been due to a variety of factors; for example,
implications for public-health issues
these species could be the ones they use most often in theirkitchens, or they could be seen as "most traditional" or culturally
Our findings could be interesting for those involved in
important, and therefore they are seen as being very important
improving health care policies targeting South-Asian migrants
in strengthening cultural identity. On the other hand, the women
in Europe, as our data provide valuable insights into concepts
may simply prefer their taste or their functional aspects such as
and views surrounding the health-giving properties of foods in
their "healthiness". These species could also have been quoted
the traditional diet within the domestic arenas. This information
also since they were in season (the survey was undertaken in the
could be crucial to both understanding the dietary habits and
spring) and were readily available in Bradford's South-Asian
improving the provision of health care through dietary consulta-
markets at the time the survey was undertaken.
tion that takes into account emic views and concepts regarding
A final major limitation of this study has been that it has been
"healthy foods". This would be especially beneficial for patients
conceived from its beginning as urban ethnobotanical survey,
with type 2 diabetes.
and it has maybe underestimated the medical anthropological
had this to say when com-
issues (e.g. emic views of illnesses and concepts of "well being")
menting on their study that focused on the barriers to physical
that are surely crucial, if we want to more holistically analyse
activity amongst people of Pakistan and Indian origin with type
phenomena related to the migrants' health.
2 diabetes in Edinburgh: "health promoters may need to workwith – rather than against – cultural norms and individual
perceptions". To this end, a culturally competent educationalintervention in patients with type 2 diabetes from ethnic minor-
This survey has shown how the consumption of traditional
ity groups living in Glasgow has been recently documented
vegetables still plays a crucial role in the dietary habits of South-
Asian migrants in Bradford, and how an important proportion
Other works have stressed the importance of culturally sen-
of the quoted vegetables are perceived as having some medic-
sitive means in primary health care of South-Asians in the US
inal properties, particularly in counteracting diabetes, whereas
others are seen just as being "good for the health". Food items
Lower rates of hospitalisation for diabetic Indian-born
with bitter or aromatic tastes are often associated with much
patients have been shown in New York City (
stronger medicinal values. If traditional cuisines are an integral
and we should perhaps seriously begin to consider the
part of complex cultural heritage systems, and if they are used by
way, for example, type 2 diabetes is managed within the health
migrant communities as a means of representing cultural identi-
institutions in our countries.
ties, it is clear that public-health researchers and policy-makers
The study that we have presented is a contribution to the dis-
need to have a much better understanding of migrants' concepts
cussion on the complex issue of migrant health (
and views regarding the health-promoting properties of tradi-
and offers a few insights that may provide a better under-
tional foods so that these can be utilized in future primary health
standing of the emic concepts of well-being and of traditional
care programmes.
practices that are believed to preserve health among migrantcommunities in Western countries.
4.7. Limitations of the study
Special thanks are due to all the South-Asian women who
took part in this survey for their enthusiasm and for sharing their
We have to underline here that the methods we chose to elicit
knowledge with the authors. Special thanks are also due to the
field data on traditionally used vegetables (free-listing) did not
Bradford School of Pharmacy at the University of Bradford for
allow us to include other categories of food plants (fruits, mush-
funding this project. We thank Lindsay Lyons for her wonderful
rooms, wild herbs, etc.) which could be important in the overall
work in editing a previous version of the manuscript.
food scenario of the South-Asians migrants living in Bradford,hence it could be said that we have overestimated the role of
the cultivated vegetables. In other words, a limitation of ourstudy is that we cannot consider the collected data on frequency
AAA, 1998. Code of Ethics of the American Anthropological Association; avail-
of consumption as absolute values and/or objective nutritional
able at: , last accessed
measurements for all the recorded botanicals. Another possi-
13th March, 2007.
ble limitation of this study is that we focused particularly on
Abate, N., Chandalia, M., 2001. Ethnicity and type 2 diabetes: focus on Asian
women's knowledge, since we know that in many human soci-
Indians. Journal of Diabetes and its Complications 17, 39–58.
Ahmed, S.M., Lemkau, J.P., 2000. Cultural issues in the primary care of South
eties women are the health-care providers within the household,
Asians. Journal of Immigrant Health 2, 89–96.
and the ones who are in charge of the domestic arena and their
Alexiades, M.N., Sheldon, J.W., 1996. Selected Guidelines for Ethnobotanical
Research: A Field Manual. New York Botanical Garden, Bronx, NY, USA.
A. Pieroni et al. / Journal of Ethnopharmacology 113 (2007) 100–110
Bagust, A., Hopkinson, P.K., Maslove, L., Currie, C.J., 2002. The projected
Johns, T., Mhoro, E.B., Sanaya, P., 1996. Food plants and masticants of the
health care burden of type 2 diabetes in the UK from 2000 to 2060. Diabetic
Batemi of Ngorongoro District, Tanzania. Economic Botany 50, 115–121.
Medicine 19, 1–5.
Jonsson, I.M., Wallin, A.M., Hallberg, H.R.M., Gustafsson, I.B., 2002a. Cul-
Balick, M., Kronenberg, F., Ososki, A., Reiff, M., Fugh-Berman, A., O'Connor,
tural foodways in Sweden: repeated focus group interviews with Somalian
B., Roble, M., Lohr, P., Atha, D., 2000. Medicinal plants used by Latino
women. International Journal of Consumer Studies, 26.
healers for women's health conditions in New York City. Economic Botany
Jonsson, I.M., Wallin, A.M., Hallberg, L.R., Gustafsson, I.B., 2002b. Choice
54, 344–357.
of food and food traditions in pre-war Bosnia-Herzegovina: focus group
Baradaran, H.R., Knill-Jones, R.P., Wallia, S., Rodgers, A., 2006. A controlled
interviews with immigrant women in Sweden. Ethnicity and Health 7,
trial of the effectiveness of a diabetes education programme in a multi-ethnic
community in Glasgow. BMC Public Health 6, 134.
Lawton, J., Ahmad, N., Hallowell, N., Hanna, L., Douglas, M., 2005. Percep-
Barth, F., 1969. Ethnic Groups and Boundaries: the Social Organization of
tions and experiences of taking oral hypoglycaemic agents among people of
Culture Difference. Allen & Unwin, London.
Pakistani and Indian origin: qualitative study. BMJ 330, 1247.
Baumann, G., 1999. The Multicultural Riddle: Rethinking National, Ethnic and
Lawton, J., Ahmad, N., Hanna, L., Douglas, M., Hallowell, N., 2006. ‘I can't
Religious Identities. Routledge, New York/London.
do any serious exercise': barriers to physical activity amongst people of
Berlin, E.A., Berlin, B., 2005. Some field methods in medical ethnobiology.
Pakistani and Indian origin with type 2 diabetes. Health Education Research
Field Methods 17, 235–268.
21, 43–54.
Borgatti, S.P., 1992. ANTHROPAC 4.0: Methods Guide. Analytic Technologies,
Leonti, M., Sticher, O., Heinrich, M., 2002. Medicinal plants of the Popoluca,
Columbia, USA.
Mexico: organoleptic properties as indigenous selection criteria. Journal of
Brett, J., Heinrich, M., 1998. Culture, perception, and the environment. Journal
Ethnopharmacology 81, 307–315.
of Applied Botany 72, 67–69.
Mackenbach, J.P., 2006. Migrant health: new challenges for European public
Burnes, C., 2004. Effect of migration on food habits of Somali women living as
health research. The European Journal of Public Health 16, 345.
refugees in Australia. Ecology of Food and Nutrition 43, 213–229.
Marcus, G.E., 1998. Ethnography Through Thick and Thin. Princeton University
Bush, H.M., Williams, R.G., Lean, M.E., Anderson, A.S., 2001. Body image
Press, Princeton, NJ, USA.
and weight consciousness among South Asian, Italian and general population
Martin, G.J., 2004. Ethnobotany: A Methods Manual. Earthscan, London.
women in Britain. Appetite 37, 207–215.
Mather, H.M., Keen, H., 1985. The Southall diabetes survey: prevalence of
Ceuterick, M., Vandebroek, I., Torry, B., Pieroni, A., 2007. The use of home-
known diabetes in Asians and Europeans. British Medical Journal (Clinical
remedies for health care and well-being by Spanish Latino immigrants in
Research and Education) 291, 1081–1084.
London: a reflection on acculturation. In: Pieroni, A., Vandebroek, I. (Eds.),
McKeigue, P.M., Marmot, M.G., Syndercombe Court, Y.D., Cottier, D.E., Rah-
Traveling Plants and Cultures. The Ethnobiology and Ethnopharmacy of
man, S., Riemersma, R.A., 1988. Diabetes, hyperinsulinaemia, and coronary
Migrations. Berghahn, Oxford.
risk factors in Bangladeshis in east London. British Heart Journal 60,
Chaturvedi, P., 2005. Role of Momordica charantia in maintaining the normal
levels of lipids and glucose in diabetic rats fed a high-fat and low-
Mellin-Olsen, T., Wandel, M., 2005. Changes in food habits among Pakistani
carbohydrate diet. British Journal of Biomedical Science 62, 124–126.
immigrant women in Oslo, Norway. Ethnicity and Health 10, 311–339.
Clifford, J., Marcus, G.E., 1986. Writing Culture: The Poetics and Politics of
Muennig, P., Fahs, M.C., 2002. Health status and hospital utilization of recent
Ethnography. University of California Press, Berkeley/London.
immigrants to New York City. Preventive Medicine 35, 225–231.
Cotton, C.M., 1996. Ethnobotany: Principles and Applications. Wiley, Chich-
Nesheim, I., Dhillion, S.S., Stolen, K.A., 2006. What happens to traditional
knowledge and use of natural resources when people migrate? Human Ecol-
Etkin, N.L., Ross, P.J., 1982. Food as medicine and medicine as food. An adaptive
ogy 34, 99–131.
framework for the interpretation of plant utilization among the Hausa of
Parsons, S., Godson, J.H., Williams, S.A., Cade, J.E., 1998. Are there inter-
Northern Nigeria. Social Science and Medicine 16, 1559–1573.
generational differences in the diets of young children born to first- and
Fagerli, R.A., Lien, M.E., Wandel, M., 2005. Experience of dietary advice among
second-generation Pakistani Muslims in Bradford, West Yorkshire, UK?
Pakistani-born persons with type 2 diabetes in Oslo. Appetite 45, 295–304.
Journal of Human Nutrition and Dietetics, 112.
Feltbower, R.G., Bodansky, H.J., McKinney, P.A., Houghton, J., Stephenson,
Pennartz, P.J.J., Niehof, A., 1999. The Domestic Domain: Chances, Choices and
C.R., Haigh, D., 2002. Trends in the incidence of childhood diabetes in
Strategies of Family Households. Ashgate, UK, Aldershot.
south Asians and other children in Bradford, UK. Diabetics Medicine 19,
Phillips, D., 2001. The Changing Geography of South-Asian in Bradford;
available at: last
Fischbacher, C.M., Hunt, S., Alexander, L., 2004. How physically active are
accessed 28th February, 2007.
South Asians in the United Kingdom? A literature review. Journal Public
Pieroni, A., 2000. Medicinal plants and food medicines in the folk traditions of
Health (Oxford) 26, 250–258.
the upper Lucca Province, Italy. Journal of Ethnopharmacology 70, 235–273.
Grover, J.K., Yadav, S.P., 2004. Pharmacological actions and potential uses
Pieroni, A., 2001. Evaluation of the cultural significance of wild food botanicals
of Momordica charantia: a review. Journal of Ethnopharmacology 93,
traditionally gathered in Northwestern Tuscany, Italy. Journal of Ethnobiol-
ogy 21, 89–104.
Hayes, L., White, M., Unwin, N., Bhopal, R., Fischbacher, C., Harland, J.,
Pieroni, A., Muenz, H., Akbulut, M., Baser, K.H., Durmuskahya, C., 2005a. Tra-
Alberti, K.G., 2002. Patterns of physical activity and relationship with
ditional phytotherapy and trans-cultural pharmacy among Turkish migrants
risk markers for cardiovascular disease and diabetes in Indian, Pakistani,
living in Cologne, Germany. Journal of Ethnopharmacology 102, 69–88.
Bangladeshi and European adults in a UK population. Journal of Public
Pieroni, A., Nebel, S., Quave, C., Munz, H., Heinrich, M., 2002. Ethnophar-
Health Medicine 24, 170–178.
macology of liakra: traditional weedy vegetables of the Arbereshe of the
Heald, A., Stephens, R., Gibson, J.M., 2006. The insulin-like growth factor
Vulture area in southern Italy. Journal of Ethnopharmacology 81, 165–185.
system and diabetes—an overview. Diabetic Medicine 23, 19–24.
Pieroni, A., Nebel, S., Santoro, R.F., Heinrich, M., 2005b. Food for two seasons:
IPK, 2005. Mansfeld's World Database of Agricultural and Horticultural Crops;
culinary uses of non-cultivated local vegetables and mushrooms in a south
available at: , last
Italian village. International Journal of Food Sciences and Nutrition 56,
accessed 13th March, 2007.
Jain, S.K., 1991. Dictionary of Folk Medicine and Ethnobotany. Deep Publica-
Pieroni, A., Price, L.L., 2006. Eating and Healing: Traditional Food as Medicine.
tions, New Delhi.
Haworth Press, Binghamton, NY, USA.
Jamal, A., 1998. Food consumption among ethnic minorities: the case of the
Pieroni, A., Quave, C.L., 2006. Functional foods or food-medicines? On the con-
British-Pakistani in Bradford, UK. British Food Journal 10, 221–227.
sumption of wild plants among Albanians and Southern Italians in Lucania.
Johns, T., 1990. With Bitter Herbs they shall Eat it: Chemical Ecology and the
In: Pieroni, A., Price, L.L. (Eds.), Eating and Healing: Traditional Food as
Origins of Human Diet and Medicine. University of Arizona Press.
Medicine. Haworth Press, Binghamton (New York, USA), pp. 101–129.
A. Pieroni et al. / Journal of Ethnopharmacology 113 (2007) 100–110
Pieroni, A., Torry, B., 2007. Does the taste matter? Taste and medicinal percep-
Riste, L., Khan, F., Cruickshank, K., 2001. High prevalence of type 2 dia-
tions associated with five selected herbal drugs among three ethnic groups
betes in all ethnic groups, including Europeans, in a British inner city:
in West Yorkshire, Northern England. Journal of Ethnobiology and Eth-
relative poverty, history, inactivity, or 21st century Europe? Diabetes Care
nomedicine 3, 21.
24, 1377–1383.
Pieroni, A., Vandebroek, I. (Eds.), 2007. Traveling Plants and Cultures. The
Sandhu, D.S., Heinrich, M., 2005. The use of health foods, spices and other
Ethnobiology and Ethnopharmacy of Migrations. Berghahn, Oxford.
botanicals in the Sikh community in London. Phytotherapy Research 19,
Povlsen, L., Olsen, B., Ladelund, S., 2005. Educating families from ethnic
minorities in type 1 diabetes-experiences from a Danish intervention study.
Scotland, N.H., 2004. Diabetes in minority ethnic groups in Scotland. NHS
Patient Education and Counseling 59, 164–170.
Health Scotland.
Ray, K., 2004. The Migrant's Table: Meals and Memories in Bengali-American
van Wyk, B.E., 2005. Food Plants of the World. Briza, Pretoria (South Africa).
Households. Temple University Press, Philadelphia.
Venkataraman, R., Nanda, N.C., Baweja, G., Parikh, N., Bhatia, V., 2004. Preva-
Rees, P., Phillips, D., Medway, D., 1995. The socio-economic geography
lence of diabetes mellitus and related conditions in Asian Indians living in
of ethnic groups in two northern cities. Environment and Planning 27,
the United States. The American Journal of Cardiology 94, 977–980.
Waldstein, A., 2006. Mexican migrant ethnopharmacology: pharmacopoeia,
Reiff, M., O'Connor, B., Kronenberg, F., Balick, M.J., Lohr, P., Roble, M.,
classification of medicines and explanations of efficacy. Journal of
Fugh-Berman, A., Johnson, K.D., 2003. Ethnomedicine in the urban envi-
Ethnopharmacology 108, 299–310.
ronment: Dominican healers in New York City. Human Organization 62,
Williams, R., Wright, W., Hunt, K., 1998. Social class and health: the puzzling
counter-example of British South Asians. Social Science and Medicine 47,
Rhodes, P., Nocon, A., Wright, J., 2003. Access to diabetes services: the expe-
riences of Bangladeshi people in Bradford, UK. Ethnicity and Health 8,
Williamson, E.M., 2002. Major Herbs of Ayurveda. Churchill Livingstone, Edin-
Source: http://www.etnobotanica.de/Pieroni%20et%20al.,%202007.pdf
Journal of Oral Rehabilitation 2008 35; 509–523 Review ArticlePrinciples for the management of bruxism* F . L O B B E Z O O * , J . VAN DER Z A A G * , M . K . A . VAN S E L M S * , H . L . H A M B U R G E R † &M . N A E I J E * *Department of Oral Function, Academic Centre for Dentistry Amsterdam (ACTA) and †Departments of Neurology andClinical Neurophysiology, and Amsterdam Center for Sleep-Wake Disorders, Slotervaart General Hospital, Amsterdam, The Netherlands
MARINE ECOLOGY PROGRESS SERIES Vol. 340: 163–171, 2007 Published June 18 Mar Ecol Prog Ser Changes in South African rocky intertidal invertebrate community structure associated with the invasion of the mussel Mytilus galloprovincialis Tamara B. Robinson1, 2,*, George M. Branch1, Charles L. Griffiths1, 2,



