Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Ppm_nov02_27-35_woessner.qxd
A Conceptual
A Conceptual Model of Pain:
Part three of this series discusses
the choice of treatment approaches
depending on the diagnosed
source(s) of pain.
by James Woessner, MD, PhD
In part one of this series,1the author de- becomes active (i.e. nociceptive pain may involvement from a herniated disc or
scribed a conceptual model of pain based
progress to neuropathic pain and then to
other physical or chemical pathology at
on electrical principles: sensors (free nerve
central pain), the physician can address
the nerve root exit from the spinal canal.3
endings), wires (axons/nerves) and the percep-
one mechanism at a time by choosing
While these distributions are usually un-
tron (spinal cord and brain). Pain was de-
treatment methods that are logically most
ambiguous, specific mapping of the sen-
scribed as either nociceptive (normal function-
effective and logistically most convenient.
sory distributions of thoracic dermatomes
ing of pain fibers), neuropathic (misfiring of
Patient perception of treatment "reason-
and the anatomic locations of the inner-
axons/nerves), or central dysfunctions (central
ableness" also plays a role in the initial
vating nerves clearly show overlapping
nervous system), the latter includes the pain
treatment adopted.
and highly individualized patterns.
pathways in the spinal cord and the brain. Part
Sclerotomal pain is deep bone pain re-
two of this series discussed methods to measure
Pain Patterns Related to
ferred from specific vertebral segments
and quantify functioning of the pain nerve
that may be interpreted as non-physio-
pathways with a view to understanding the un-
Having pathology is not the same as hav-
logical. Bone pain may be either local or
derlying pathology causing the pain.2
ing pain from that pathology. Without vis-
referred from ipsilateral spinal segments.3
ible tissue changes, there may not be a pe-
Pain referred from tendinous and/or
ripheral pain generator, leaving neuro-
ligamentous interfaces with bone surfaces
The concept that pain results from me-
pathic and/or central pain as the proba-
has no specific name that may also be in-
chanically- and chemically-caused physical
ble cause. There could also be a micro-
terpreted as non-physiological. Hackett4
changes that become more and more dif-
scopic pathology and/or local metabolic
mapped pain referred from ligamentous
ficult to reverse is well-accepted through-
reason. Ultimately, there must always be
and tendon attachments to bones.
out Medicine. With the passage of time, the
a mechanism whereby some pathology or
Drs. Travel and Simons5,6 have provid-
reasons for the pain also become multi-fac-
dysfunction causes the perception of pain.
ed physicians and patients with detailed
torial and overlapping, as well as more dif-
There are, however, a multitude of pain-
maps of referred pain patterns from my-
ficult to cure. Thus, early treatment is bet-
pathology referral patterns. Most physi-
ofasical trigger points. While individual
ter to avoid permanent physiologic and
cians only recognize dermatomal pat-
variations certainly occur, in general,
structural changes and facilitate a cure.
terns; there are also sclerotomal, myofas-
these patterns of referred pain can be rec-
While the pain mechanism(s) may be-
cial, viscerotomal, thermatomal, my-
ognized in physician practice, and may
come more complicated over time,1,2 as
otomal, as well as other referral patterns.
sometimes be incorrectly referred to as
more than one of the basic mechanisms
Dermatomal pain suggests nerve root
"non-physiologic" pain patterns.
Practical PAIN MANAGEMENT, Jan/Feb 2003
Likewise, the pain referral patterns of pathology in the in-
table, complex, and difficult to cure over time. Anti-nociception
ternal organs are well-known across multiple field of medicine.
can be a dysfunctional result in any type of pain.
Of course, there is an embryologic basis for these fairly consis-
Environmental influences are certainly recognized to influence
tent patterns of pain.5,6
pain. Cold, wet days make neuropathic pain (including CRPS,
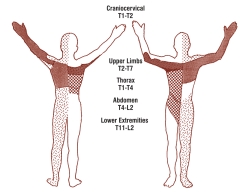
There are also thermal patterns of pain, which are probably re-
myofascial, and fibromyalgia), worse. Just as old arthritics often
lated to the distribution of sympathetic nerves (see Figure 1).7
comment that they "can feel" weather changes in their "bones,"
Butler8 has mapped referred pain from the spinal dura, which
patients with neuropathic conditions often complain of more
is also probably related to stimulation/irritation of the sympa-
achy pain during bad weather. If consistent across these types of
thetic C-fibers on the dura. Pain referred from the spinal dura
pain patients, this phenomenon would support the concept that
is reminiscent of thermatomes in being diffuse, but these refer-
myofascial pain and fibromyalgia have, at least, a neuropathic
ral patterns are unique.
Bonica and Loeser describe "myotomal" pain as involving
Pre-morbid and secondary psychological/psychiatric condi-
problems with the fascial tissue planes that surround muscle
tions do often complicate diagnosing a pain condition. While
groups.3 While "myotomal" may not be the correct description,
depression may only sometimes be considered a cause of pain,
when muscles were injected with hypertonic saline, which is an
the converse is certainly true. Dissatisfaction, psychosocial emo-
experimental substance known to produce pain, the above-
tional stress and desire for secondary gain can occur concomi-
mapped patterns of referred pain emerged.
tantly with objective physical pathology. In other words, the pa-
Sometimes the myofascial pain referral patterns follow der-
tient may present with a chronic condition that, in some ways,
matomes, to some degree.9 Dermatomes are somatic sensory
is exacerbated by a new injury.10
nerve distributions whereas trigger point pain referral patterns
Basic individual personalities and cultural background have
are more related to sympathetic C-fiber distributions.
a significant affect on the perceived degree of pain and dys-
There is much to be investigated and considered before an
function, i.e. the patient's reaction to the pain. Chronic pain
integrated theory really useful to pain management can be ad-
conditions are also often exacerbated by the withdrawal of fam-
ily and friends support.10 Financial pressure to pay doctor's bills
These different pain referral patterns may even occur simul-
and maintain life generates stress, raises cortisol levels and con-
taneously. If the physician does not pick out the correct primary
sequently lowers pain thresholds.
pathology, treatment is — at best — a hit-or-miss "shotgun" ap-
Pain and discomfort can essentially cause fatigue and sleep
proach. This approach is demonstrated on a daily basis as many
dysfunction, which further slows healing and increases suffer-
physicians routinely — but consistent with the standard of care
ing. Metabolic diseases, such as diabetes, may either be a pri-
and training they've received — prescribe muscle relaxants,
mary cause of pain, contribute in varying degrees to the pain,
pain-killers (opioid/acetaminophen), NSAIDs (non-steroidal
may exacerbate a psychological component or, in other cases,
anti-inflammatory drugs) and sleeping pills to patients in acute
may have nothing to do with the pain for which the patient
and chronic pain.
It is important to note that "curing" the pain, as opposed to
"masking" it, requires a specially trained physician to precisely
and effectively decide the primary cause of a patient's pain prob-
As presented in the second article of this series, the pain fibers
lem and to pick the best and most effective treatment early in
can transmit — or be perceived as transmitting — less or more
their care. This exercise is the essential first step in deciding ona theoretically-based and pragmatically-possible treatment plan.
Interestingly enough, these different pain etiologies and pat-
terns are most directly helpful in dealing with nociceptive pain.
In other words, these pain sources and referral patterns basical-ly represent normal neurophysiologic functioning and, by andlarge, provide the patient and the physician with useful infor-mation in determining a good working diagnosis for nociceptivepain. However, actual clinical presentations are usually morecomplex.
Complicating Factors
While somewhat arbitrary, acute and chronic pain are concepts
that must be considered and are useful in the sense that changes
of real consequence occur over time. There are typically many,
more complex, and permanent changes that do occur. Certain-
ly, most physicians have seen the very visible changes that can
occur in the natural progression of CRPS or RSD.
Neuropathic changes can also occur with CRPS and other pain
FIGURE 1: Hooshmand7 has coined the word "thermatomes" to describe
conditions as illustrated in the 2nd of this series.2 If efferent
referred pain patterns related to the circulatory distribution of sympa-
pathways are either damaged or are responding in a reflex man-
thetic nerves. These relatively amorphous distributions are consistent
ner to aberrant afferent signals, then easily visible anatomic and
with the observation that these C-fiber nerve pathways end up seeing
structural changes can occur. These changes become more no-
pain "through fogged glass."
Practical PAIN MANAGEMENT, Jan/Feb 2003
signals than normal (damaged/dead and
thetic C-fibers, making the procedure less
CRPS likely involves all three, i.e. struc-
irritated fibers, respectively). In addition,
tural tissue changes that stimulate noci-
there can be mixture of functional levels
How can one really predict in each in-
ceptors, malfunction of small pain neu-
in a population of axons; the summation
dividual case? Scientific results can be
rons, and central neuronal changes con-
of hypo- and hyper-function can result in
supportive, but individualized, artful de-
sistent with central hypersensitivity.1,2
average function that mimics normal
cisions are the modus operandi through-
out Medicine, particularly in Pain Man-
Treating Nociceptive Pain
Small pain nerve (A-delta and C-fiber)
agement. Protocols are to be viewed as
Disease, pathology and pathophysiologi-
pathology should intuitively have several
guides — not the last word.
cal processes cause mechanical or chem-
etiologies. Sudden trauma to a body part
ical pain, which is usually nociceptive.
would seem to also have the potential to
Physicians are most skilled at identifying
damage by crushing the small pain
No matter how complex the pain problems
nociceptive pain as the pain-causing
nerves, resulting in acute and then chron-
of any individual patient, patterns of
pathology. Unless the nerves themselves
ic compressive neuropathy. An acute com-
pathology do emerge and treatment op-
are damaged or central pathways physio-
pressive neuropathy may cause physical
tions can be chosen. A framework must be
logically altered, curing or removing the
and chemical changes that can become a
developed for approaching a pain problem
cause is the physician's primary concern.
chronic non-compressive and/or traction
starting with diagnoses. Among these di-
When it comes to cure, traditional al-
neuropathy. Chronic repetitive rubbing
agnoses, the physician must decide which
lopathic physicians are most successful in
can end up causing nerve dysfunction
is primary, causative and/or dominant.
treating nociceptive pain problems — as
from similar physical and chemical con-
long as neuropathic and central problems
do not develop too quickly. For instance,
These physical insults often cause local
No matter how complex
if a benign cyst is pressing on a nerve root,
chemical changes manifest by swelling,
it can be surgically removed and we would
redness and hotness, i.e. inflammation.
expect resolution of the pain — unless
Inflammation causes certain chemicals to
neuropathic and/or central pain prob-
the pain problems of any
be released in the damaged tissues. There
lems have developed.
are numerous such identified chemicals; a
Neuron blockade and pain-killers of all
few examples are prostaglandins, periph-
sorts may be used initially to create "win-
eral serotonin, kinins, histamines, etc.11
individual patient, pat-
dows of opportunity" for cure. Chronicuse of pain-killers is condoned and med-
The Problem with Treatment Protocols
ically honorable once the physician and
Treatment protocols, as well as scientific
the patient have made an honest effort to
terns of pathology do
experimental results, are problematic be-
cure and to recover, respectively.
emerge and treatment
cause each assumes that there is a range
The following presents some of the au-
of normal that must apply to every indi-
thor's experience as an outpatient physi-
vidual pain patient, whereas aspects of
cal medical physician in treating noci-
each individual patient's problem are ab-
solutely unique. Pain is usually different
RICE: Rest, Ice, Compression and El-
every day, and it changes unpredictably
options can be chosen.
evation are the elements of the tradition-
over the course of the day.
al approach in caring for acute sprain/
It is well known that even when it comes
strains. The physician and the patient are
to the mu-receptors in the spinal cord,
By and large, most acute pain is noci-
basically treating swelling, redness, hot-
there are at least 10 types and each indi-
ceptive. On the other hand, trauma can
ness and pain. These modalities result in
vidual has different proportions of these
also damage the small pain nerves caus-
less pain and expedite recovery. The ex-
types. Obviously, it is impossible to pre-
ing immediate neuropathic problems. For
perienced physician may also include
dict for an individual pain patient which
example, the perceptron/central patholo-
opioid will be effective and at what dose;
gy for phantom pain, resulting from am-
Physical Therapy: All of the PT
different individuals will have widely dif-
putation or central disconnection, is
modalities, including passive manual
ferent opioid requirements for their pain.
probably established at the instant of trau-
therapy and therapeutic exercises, are the
Further, opioid requirements will change
ma, but realized or perceived days, weeks,
best curative approach. All sorts of pain-
over the course of the day, every day, re-
or months later.
killers and injections may very well pro-
quiring more or less to control pain.
Chronic pain most likely, but not nec-
vide windows of opportunity for these ef-
Treatment history can also have infinite
essarily, involves all three types of pain —
forts to be effective. The unifying princi-
possible courses and happenings. If mul-
nociceptive, neuropathic, and central.
ple of Physical Medicine — i.e. tissue re-
tiple previous chemical blocks have pre-
Varying degrees and patterns of these dys-
molding — is facilitated and achieved,
ceded efforts with electromedical nerve
functions occur to result in the different
however, by physical therapy.
blocks,12 the resultant scar tissue from the
pain conditions. In some cases of arthri-
Therapeutic Exercise: The most ef-
chemicals around the stellate ganglion
tis, neither neuropathy nor central dys-
fective tissue remolding technique is ther-
will likely interfere with penetration of the
function occurs. Fibromyalgia could be
apeutic exercise under professional Phys-
electric current to the underlying sympa-
completely central, but not psychogenic.
ical Therapist supervision or at home. In-
Practical PAIN MANAGEMENT, Jan/Feb 2003
fluencing the micro-environment of the
nerve pathways makes sense and many
probably not stimulators at all but, more
tissue planes of the body by moving tis-
patients are happy with the results. Radio
likely, continuous neuron blockade of the
sues with respect to other tissues, possibly
frequency ablation is the preferred way to
pain nerve pathways in the dorsal
in conjunction with other procedures and
burn or cut the offending nerves. Recur-
columns. If these signals were indeed stim-
therapies, is the key to cure. These exer-
rence, on the other hand, happens fre-
ulating, they would be stimulating pain.
cises include stretching, strengthening
quently. Three possibilities come to mind:
The classic gate theory does not apply in
and endurance training-type of move-
1) a new transmission pathway develops,
the author's opinion. Patients with SCSs
ments that vary in intensity, repetitions,
2) local neuropathology develops from
seldom state that pain relief in 100%; they
sets, duration and session frequency.
the cut nerves, and/or 3) delayed central
more often describe the sharp pains as
Manual Therapies: Medical myother-
hypersensitivity sets in.
being reduced but with the nagging, burn-
apy, deep soft tissue massage, rolfing,
IDET: Intradiscal electrothermal re-
ing and aching pains remaining.
neural flossing,8 the Gunn technique13
duction of herniated nucleus pulposus is
Intrathecal Drug Pumps: Distribution
and numerous other strengthening exer-
a procedure that would seem to reduce
ports are surgically placed in the epidur-
cise techniques can be artfully integrated
the morbidity of full-blown surgical pro-
al space, where combinations of various
with other above-mentioned treatments
cedures. However, the author's experi-
painkillers and muscle relaxants are de-
for resolution of a patient's pain.
ence has been that third party payors have
livered. In the author's opinion, these
Chiropractic Care: Chiropractic care
resisted accepting this procedure. In the
pumps are probably overused. Instead,
usually includes modalities and thera-
situations that IDET is unsuccessful, the
optimized use of slow release opioid
peutic exercise identical to those used in
problems may be due to microscopically
preparations and muscle relaxants are
physical therapy. Unique, but not propri-
etary, aspects of chiropractic care include
When nothing can be done to correct
applied kinesiology, activator adjust-
Disease, pathology and
the underlying cause, the pain can, of
ments, high-velocity and low-velocity
course, be dysfunctional and require tra-
joint manipulations of various descrip-
ditional and well-accepted pharmaceuti-
tions and the use of multiple modalities.
cal pain control.
Chiropractic can be very a useful facet ofa multidisciplinary pain management ap-
The Pharmaceutical Approach
These pharmaceutical suggestions are the
Injections: There are injections done
processes cause
author's preferences based on the known
primarily to reduce pain, to reduce in-
mechanisms of actions (pharmacokinet-
flammation or to stimulate natural
ics) and location of action inside the body.
processes. Local anesthetics, catabolic
Oral Opioids: Opioids are probably
mechanical or chemical
steroids and proliferative agents are used,
the safest of all the pain-killers. However,
pain, which is
respectively. The efficacy of the injections
for those patients suffering from neuro-
described below depend on the correct-
pathic pain alone, pain management
ness of the diagnosis, the physician's un-
health care professionals recognize that
derstanding of the utility and effect of the
opioids merely "take the edge off," while
injected substances, and finally whether
many patients recognize no help at all.
the injected substance reaches the target
usually nociceptive.
For this specific population, patients re-
porting that opioids "take the edge off "
Local anesthesia ideally blocks the pain
may, in fact, be potentially addicted. On
and provides a window of opportunity for
rough surfaces remaining after disc ma-
the other hand, opioids typically do le-
sleep, reduced stress, and various thera-
terial is destroyed and possibly from the
gitimately benefit those patients who have
peutic activities.
resulting reduced disc height. This as-
nociceptive pain (with or without neuro-
Catabolic steroids, by definition, break
sumes that the diagnosis was correct in
pathic pain). The author's professional
down tissue. If the physician does not want
the first place since discography is often
experience confirms that when the noci-
tissue breakdown, steroids should not be
not predictive of the causative pathology.
ceptive pain patient is freed from the dis-
used. Reducing abject inflammation
Surgery: Whole textbooks are written
tractions of the pain, there is commonly
and/or softening pain-causing scar tissue
about lumbar surgery. Short-term out-
an improvement in mental function.
are reasonable goals for steroid injection. comes have been reasonable, but long-
NSAIDs: Non-steroidal anti-inflam-
Proliferative agents are intended to in-
term results have been disappointing. Mi-
matory drugs (both COX-1 and COX-2) in-
crease healthy collagenous tissue. Pro-
crodiskectomy has about the same draw-
hibit inflammation and provide analge-
lotherapy is beginning to receive scientif-
backs as IDET. Metaphorically speaking,
sia.16 Inhibiting the inflammatory cascade
ic support14 and wider recognition among
laminectomies and various types of fusion
may be beneficial to prevent tissue dam-
surgeries are really major trauma. Like
age for the first few days. During more ad-
Radio Frequency Ablation: If periph-
many things in Medicine, sometimes a
vanced healing phases, a normally func-
eral pathology is chronic, purely noci-
poisonous medication or a traumatic pro-
tioning inflammatory process is necessary
ceptive, without removable pathology
cedure is used to benefit when other, more
for the best possible tissue recovery. While
and without neuropathic or central dis-
conservative, approaches fail.
the NSAIDs are not recommended beyond
ease, burning or cutting the offending
Spinal Column Stimulators: SCSs are
the first days of an acute injury, they may
Practical PAIN MANAGEMENT, Jan/Feb 2003
be useful in clearly chronic disease for
Pertofrane®). TCAs have data to support
tagonizing actions at the presynaptic ter-
analgesia, but the side effects of GI prob-
some effcicacy in fibromyalgia. The SSRIs
minal, neither nociceptive nor neuro-
lems, kidney dysfunction, and possibly
include fluoxetine (Prozac®), paroxetine
pathic pain signals should be perceived
heart problems with the COX-2 NSAIDs,
(Paxil®), citalopram (Celexa®), sertraline
must be closely monitored — especially in
(Zoloft®) and venlaxine (Effexor®). The
Since the physician's best efforts are fre-
elderly and immune-compromised pa-
biochemical precursor to Serotonin is the
quently unsuccessful, understanding of
tients. Ibuprofen and Naproxen are over-
amino acid, tryptophan, which is available
pain transmission must be less than per-
the-counter NSAIDs.
in turkey meat. Supplementation may be
fect. What is known is that the pain signals
Other OTC Meds: Acetaminophen and
reasonable in those depressed, not sleep-
are weakened by encephalin-induced
aspirin are the main remaining OTC
ing, and with resulting exacerbated pain.
dynorphin activity in the spinal cord.
pharmaceuticals. Both are underappreci-
Anticonvulsants and Antiarhythmics:
Dynorphin activation of kappa receptors
ated yet are effective pain-killers and can
Rowbothan & Petersen19 only mention
on inhibitory interneurons causes the re-
be excellent low level pain control agents
one antiarhythmic, i.e. mexiletine. It
lease of GABA, which hyperpolarizes dor-
for mild pain, depending on the individ-
along with carbamazepam (Tegretol®),
sal horn cells and inhibits further trans-
ual patient. Each can be used on a daily
gabapentin (Neurontin®), lamotrigine
mission of the pain signal. This latter
basis for long periods. However, chronic
(Lamictal®), phenytoin (Dilantin®), topi-
mechanism is especially important in
use of acetaminophen can cause liver
ramate (Topamax®) and valproic acid (De-
modulating visceral pain. Medications
and/or kidney failure, while chronic use
pakote®) can be considered membrane-
that mimic the efforts of endorphins and
of aspirin can cause acute GI bleeding.
stabilizers in the sense that most of these
encephalins are the mainstays of chronic
Muscle Relaxants: Lioresal (Baclofen®),
pain therapy. Newer drugs that mimic or
carisoprodol (Soma®), chlorzoxazone
potentiate the effects of GABA or alpha2-
(Paraflex®), cyclobenzaprine (Flexeril®),
Remembering that neuro-
receptor agonists have made it possible to
diazepam (Valium®), methocarbamol
target therapy for chronic pain syndromes
(Robaxin®), orphenadrine (Norflex®) and
more specifically than in the past."20
tizanidine (Zanaflex®) are all commonly
Most utilized pharmaceutical mecha-
pathic pain is related to
used muscle relaxants.17 Lioresal works at
nisms are basically antinociceptive in na-
the GABA receptors discussed below and
ture. It may be that all of the antagonists
could, via antinociceptive mechanisms,
must be supplied simultaneously. Further,
reduce reflex muscle contraction. Cariso-
nerve (wire) dysfunction
Brookhoff20 suggests more complex in-
prodol is preferred by many patients as it
teractions involving sympathetic and
often helps with sleep, yet poses problems
parasympathetic nervous systems that,
due to its addictive characteristics. Cy-
being poorly understood at this time, are
itself, curative treatment
clobenzaprine is related to the tricyclic
without pharmaceutical approaches.
must, therefore, focus on "
antidepressants and probably works cen-trally and it can also be useful for sleep.
Treating Neuropathic Pain
The author seldom uses chlorzoxazone,
Radiological imaging of the spine and
methocarbamol and orphenadrine, each
brain are rarely helpful in determining
of which is in a pharmodynamic class of
neuropathic, central, or even nociceptive
its own. Tizanidine (discussed in a subse-
reversing that pathology.
pain. Nerve damage can occur via an in-
quent section) works at receptors on pe-
finite number of mechanisms, and result
ripheral nerves, spinal cord neurons and
in several outcomes, i.e. hyperesthesia
central neurons.18
medications reduce ectopic extraneous
and/or hyperalgesia, paresthesias and/or
Lidoderm: While there are analgesic
nerve firing by blockade of sodium chan-
allodynia, or hypoesthesia; the ultimate
creams, Lidoderm, at present, is the only
nels. Clonazepam is a benzodiazepine
hypoesthesia is the complete inability to
topical preparation that comes as a patch.
that is included by Rowbothan and Pe-
experience any pain at all. Remembering
When using all topicals, the physician
tersen, but works mostly like diazepam.
that neuropathic pain is related to nerve
must remember that the depth of the pain
Carbamazepam is the only one of these
(wire) dysfunction itself, curative treat-
nerves can be a problem; in other words,
indicated as safe and efficacious for pain
ment must, therefore, focus on reversing
these preparations work better when
by the FDA. Tegretol and Neurontin may
causative pathology is near the skin sur-
also work synergistically and are also used
Other than trying to mask the pain by
face. The chemicals do not penetrate or
for mood disorders.
means mentioned above, nutritional ap-
diffuse in effective quantities deeper, be-
proaches should be primary and synergis-
cause the circulatory system absorbs and
Sites of Pharmaceutical
tic. Omega fatty acids (6 to 3) in the ratio
gradually disperses the active ingredients
of 4 to 1 have been shown to optimize
as the chemical penetrates deeper.
Pain signals from free pain nerve endings
nerve function. Since Omega fatty acids
SSRIs and Other Antidepressants: Tri-
and from dysfunction peripheral nerves
are the building blocks for nerve mem-
cyclic antidepressants (TCAs) include
are conveyed to the perceptron through
branes, we would expect that supplement-
amitriptyline (Elavil®), imipramine
the synapse of the peripheral nerve on the
ing a neuropathic pain patient's diet would
(Tofranil®), nortriptyline (Pamelor®, Aven-
dorsal horn of the spinal cord. Theoreti-
be a reasonable approach to suggesting
til®) and desipramine (Norpramine®,
cally, if those signals are blocked by an-
cure. We would expect 4 to 6 months to
Practical PAIN MANAGEMENT, Jan/Feb 2003
elapse before the patient or the doctor may
natural-healing and anti-immune. It is
quately educated the pain patient. Even
see any noticeable improvement.
well known that increased cortisol lowers
so, a couple of examples may be instruc-
In a previous article,12 the author re-
pain threshold. Psychophysiological fac-
tive at this juncture.
ported that medium frequency, especial-
tors with complex interactions are obvi-
Complex Regional Pain Syndrome
ly 20,000 Hz, alternating current across a
ously involved in pain perception.
(CRPS), previously named Reflex Sympa-
tissue culture resulted in utilization of
The most logical treatment approach is
thetic Dystrophy (RSD) usually starts with
cyclic AMP.21 Understanding the role of
to use methods that directly affect neu-
neuropathology of the A-delta and C-
cyclic AMP suggests that normalization of
rons in the central nervous system. Tran-
fibers caused by acute or repetitive trau-
nerve function can occur by stimulating
scranial and body stimulation, auricular
ma. Damage to efferent nerves causes vis-
anabolism. Masking neuropathic pain can
and traditional acupuncture, reflexology,
ible physical changes that are well-de-
also occur via electric neuron blockade.
applied kinesiology, yoga, imagery, and a
scribed in CRPS/RSD. Also many researchers
In both cases, we would expect that the
whole range of psychological techniques
have noted intracranial changes,24 which
unmyelinated C-fibers would benefit
are valid possibilities.
are most likely subcortical. CRPS/RSD is a
more than the A-delta fibers.
Nutritionals, such as gingko, may also
non-standard, variable disease, and as
Supplemental to the above approach-
play a role.22,23 We would expect nutri-
stated, varies among individual patients.
es, is the use of so-called membrane sta-
tionals to be the building-blocks of repair
Even before the name of Reflex Sympa-
bilizing medications; these medications
and normalization of function. Since sub-
thetic Dystrophy was changed to Complex
appear to stabilize nerve membranes by
tle nutritional deficiencies or medicinal
Regional Pain Syndrome, it has been ap-
antagonizing signal transmission at spe-
needs take time to develop, we would also
preciated that these neuropathies involve
cific receptors on pain nerves to prevent
expect that repair would likewise take
more than one type of nociceptive fiber.
hyperactive flow related to transmission
months to years (see the section on the
Fibromyalgia is another common
of pain signals. These medications are
role of nutritionals).
chronic disease which, in the authors
mostly anticonvulsants, but also include
Sometimes psychiatric conditions, such
opinion, has probable involvement of the
tricyclic antidepressants and antiarrhyth-
as depression, anxiety and Post-Traumatic
three pathologies supported by the pain
mics. Zonegran blocks sodium, T-type cal-
Stress Disorder (PTSD) are the cause of pain
model described in this series. However,
cium and K-evoked glutamate receptors.
and discomfort. It has been scientifically
because of the dynamics of post-traumat-
Neurontin (gabapentin) and Gabatril are
confirmed that depression, at least, can be
ic fibromyalgia and the patchiness that
reported by Brookhoff20 to have actions
correlated to central neurochemical
the author has observed, it is suggested
unrelated to GABA receptors shown above.
changes. Such chemistry can be modulat-
that fybromyalgia probably starts periph-
With knowledge of the nerve fiber type
ed via Selective Serotonin Re-Uptake In-
erally. But fibromyalgia also surely has
involved, specific, focused treatments
hibitors (SSRIs) and other antidepressants.
central components because of the asso-
may be possible. Neuropathic pain, as it's
Pharmaceuticals that pass the blood-
ciated cognitive and emotional sequelae
usually used, refers to a burning, aching,
brain barrier may also have potential for
and concommitant symptoms.25
non-localized pain which points to in-
cure, but so far appear to only suppress
While not curative, Zanaflex® has been
volvement of the C-fibers. The usual
the pain sensation. In the same sense of
found by the author to be the best phar-
treatments are pharmaceutical. Thus,
membrane stabilization, anticonvulsants
maceutical for directly treating combined
when the area pain is regional in nature,
and other pharmaceuticals mentioned
nociceptive, neuropathic and central
the physician must, in consultation with
above, have also been documented to be
causes of pain with the least side-effects.
the patient, decide, depending on the
useful for treating pain with central com-
Zanaflex® is a basic alpha2 adrenergic ag-
character of the neuropathic pain pres-
onist active in the polysynaptic pathways
ent, whether bathing the whole body in a
Because mechanisms are still in the
in the spinal cord and in the locus
pharmaceutical, the possibility of de-
early stages of discovery, psychogenic
ceruleus and is unique in its widespread
pendence and the expense are worth the
causes of pain may very well be eventual-
sites of action.18
minimal general pain relief and/or pain
ly understood to be either chemical or
relief in a single region.
anatomic (neuronal) changes in central
Tissue Remolding and Tissue
pain perceptor systems.
Treating Central Pain
Physical Medicine includes numerous
Central pain, according to the author's
Treating Combined Pain
techniques to remold tissue. These in-
definition, is any pain resulting from dys-
As indicated previously, almost all chron-
clude modalities and body movement im-
function of neurons of the central nerv-
ic pain is a combination of the nocicep-
plemented by both active and passive
ous system, i.e. the brain and the spinal
tive, neuropathic and central pain with-
means to change the micro-environments
cord. Thalamic pain and phantom pain
out a clear single pain generator. Books
— both intra-cellular and extra-cellular.
fall in this category. Perceived body pain
have been written considering all aspects
Tissue remolding, in a microscopic
in complete spinal cord injured patients
of various pain syndromes, yet protocols
sense, is the changing of the microenvi-
must be central in origin and mainte-
and set recipes are too restrictive for the
ronment. This phenomenon is mostly col-
infinite variations found in patients. Each
lagen remolding. However, other aspects
Because elevated cortisol is known to be
patient is an unique individual, whose
of this microenvironment are likely in-
anti-inflammatory in the human body, we
condition varies from minute to minute.
volved. Temperature, pH and other
would thus also expect that any stress
There is no substitute for a knowledge-
chemical parameters almost certainly
causing increased cortisol will also be anti-
able, flexible physician who has ade-
come into play. Nutritional building
Practical PAIN MANAGEMENT, Jan/Feb 2003
MANAGING CHRONIC PAIN IN TEN EASY STEPS
Be Realistic. Be honest with yourself and learn all you can about your physical condition. You may well have to deal with the fact
that your will need to deal with pain every day. Dealing with anger, frustration and change is an important part of the process.
Get Involved. Take an active role in dealing with your condition. Find out about all options available to you and move from a
passive to an active role in your healthcare. You may wish to look at non-medical options for support and help. Alternatives
such as acupuncture, homeopathy and looking at diet may be useful.
Learn Relaxation and the Value of Distraction. This isn't about booze and smokes! Learning to breathe and relax properly
distracts your mind and gives mind and body a break from the suffering associated with pain.
Recognize Thoughts and Feelings. The mind affects the body and the body affects the mind. Identifying your thoughts and
feelings is vital if you want to change how you relate to your pain.
Safe Movement. Safe movement combined with deeper breathing can improve mobility and make you feel more positive.
Set Priorities. With limited energy and mobility, it is important to look at what matters in your life. Ask yourself: "What do I
want?" Never mind the "should's".
Set Realistic Goals. Break big tasks into smaller more manageable steps that you can achieve. Pace yourself; continually
review pain and energy levels relative to activity. you will feel more in control.
Know Your Basic Rights. You have the right to be treated with respect, to say "no" without guilt, to do less than humanly pos-
sible.
Communicate. Communicating clearly and effectively with family and friends and colleagues reduces anxiety, tension, stress,
and suffering. Learning how to get your needs med is an important part of pain management.
STEP 10 Rediscover Hope. By using these strategies you will find that you can: Regain control; Increase your sense of well-being; Step
out of the pain-tension-anxiety-stress-cycle; Begin to get your needs met; Lessen suffering.
TABLE 1. Self-help steps in managing chronic pain developed by the Pain Association Scotland.
blocks, as well as fibroclastic and fibrob-
and/or hypoactive, depending on the
fibers in tissue planes and around other
lastic cells, must be present.
axon within the "cable" of the whole nerve.
structures such as nerves. Because these
Circulation changes affect microenvi-
These tissue plane micro-environments
are unmyelinated, it makes sense that
ronmental chemistry. If circulation is
may be mobilized by stretching, neural
electrical energy, as a treatment modality,
modified, then it's fairly certain to change
flossing,8 strengthening, manual therapies
would more likely penetrate these nerves
the biochemical environment of the pe-
to include various massage techniques,
and thereby provide immediate pain re-
ripheral areas involved. More blood
rolfing, other deep soft tissue techniques,
lief while promoting recovery of any C-
means more nutrients and more disper-
craniosacral techniques, etc., and thera-
fiber pathology and malfunction.
sal of metabolites, and vice versa. Like-
peutic exercise. The unifying principle of
Changes occur even at the nociceptor
wise, microenvironmental chemistry af-
physical medicine for the cure of soft tis-
terminal level in any chronic pain condi-
fects circulatory changes thereby illus-
sue pathology is tissue remolding.
tion. Brookhoff20 gives a detailed descrip-
trating the complex interrelationships.
tion, including the production/release of
Efferent sympathetic C-fibers control
Chronic Pain in Perspective
natural painkillers in the chronic pain sit-
peripheral microenvironmental circula-
Chronic pain includes CRPS/RSD, fi-
uation. Methods to naturally stimulate
tion. This makes microenvironmental
bromyalgia, central pain conditions and
the release of native pain-killers such as
conditions directly related to local and sys-
any pain that is present for long periods
endorphins and enkephalins would seem
temic sympathetic nervous system func-
of time, is not likely to resolve, and man-
to be an ideal way to promote natural pain
tion — via reflex actions or centrally. This
ifests in anatomic/physiologic changes.
control. Brookhoff also shows how potent
can be understood starting first with cen-
Chronic pain of any kind almost certain-
inflammatory and vasodilating agents are
tral control of the peripheral circulation.
ly includes combinations of the above
released following prolonged sensitiza-
Microenvironments can be intracellular,
pathologies, simply because one can pre-
tion of the cells in the dorsal horn.
where metabolism is controlled or regu-
cipitate another.
Successful treatment, of course, de-
lated by second messengers, or extracel-
In general, chronic stimulation of no-
pends on the exact cause. However, even
lular. The most important extracellular
ciceptors results in permanent physiolog-
with clear peripheral pathology causing
micro-environments are the tissue planes
ic and microanatomic changes. While
nociceptive pain, most of the treatments
between tissue systems. As stated above,
acute pain response is in the nociceptor
mentioned above probably have less
these microenvironments contain the A-
terminal and is facilitated by glutamate,
probability of providing a complete cure
delta and C-fibers that carry pain signals.
chronic pain is more involved and com-
because of the neuropathic and central
If these micro-environments are altered,
plex. Most chronic conditions include
logically we would expect that the fiber
malfunctioning sympathetic C-fibers. It is
In reality, the only proven approach for
would become hyperactive (irritated)
well known that there are numerous C-
chronic pain to date is counseling the pa-
Practical PAIN MANAGEMENT, Jan/Feb 2003
tient to deal with the pain and develop-
vides a rationale for the neuropathy of
the stellate ganglion — will likely interfere
ing a pain management plan involving
cobalamin deficiency. Odd-chain fatty
with penetration of electric current to the
long-acting opioids.26 After all else has
acids would build up in membrane lipids
sympathetic C-fibers by any subsequently
failed, covering up the pain in the con-
of nervous tissue, resulting in altered
attempted electromedical nerve block.
text of a chronic pain program is an ac-
myelin integrity and demyelination, lead-
Note that electromedical nerve blocks of
cepted and honorable approach to im-
ing eventually to impaired nervous system
the stellate ganglion are more difficult to
proving the quality of life of the pain suf-
confirm than chemical blocks, in part be-
ferer. A comprehensive self-help program
It is reasonable to postulate that the use
cause the Horner's sign is subtler.
for managing chronic pain, developed by
of nutritionals effects the entire pathway,
In the face of allodynia and hyperes-
the Pain Association Scotland,27 is pre-
including the peripheral nervous system
thesia, electromedical treatments and
sented in Table 1.
and the central nervous system — all the
other therapy may also directly help de-
way through the spinal cord and into the
crease disuse atrophy and cure some dis-
The Role of Nutritionals
eases that otherwise cause muscle atrophy,
Proteins, carbohydrates, fats, vitamins
skin color changes, and functional de-
and minerals are all building blocks for
The Role of Electric Medicine
creases in strength and ROM.
tissues and cells. Nutritional precursors
That there are electrical aspects to human
are necessary to allow the body to metab-
physiology is well-accepted. Note that
The Role of Complementary/
olize appropriate bi-products for cure and
EKG, EEG, EMG, nerve conduction stud-
Alternative Medicine (CAM)
normalization of function and structure.
ies, evoked potentials, pace makers,
All kinds of acupuncture (traditional, au-
Basic nutrition promotes good health.
ricular and electrical), reflexology, koryo
However, there is another approach that
(Korean hand acupressure), etc. likely re-
can be used separately or concomitantly.
sult in reprogramming neurons to normal
In the face of disease, medicinal doses are
function. These techniques, when they
necessary and useful. This approach is to
work, would then logically work better for
encourage the patient to supplement his
central nervous system pain dysfunctions.
are necessary to allow
or her diet with so-called building block
Herbal approaches are by and large not
proven in a Western scientific sense. The
Glucosamine sulfate is a known build-
role and value of nutritional is gradually
ing block for collagen. Besides being a
the body to metabolize
finding scientific support, but the "proof "
logical nutritional for arthritis, it could
is slow in coming.
play a role in neuropathic pain, because
A recently published 656-page refer-
collagen has been shown to form the
ence volume deals specifically with the
appropriate bi-products for
sheaths around nerves — the micro-envi-
subject of using Oriental Medicine tech-
cure and normalization of "
ronment of nerves.
niques to treat pain.29 The pain etiology
Omega fatty acids have roles in the
is based on the Chinese concepts of ex-
health of many body systems. Here, we
ogenous factors.
are interested in its presence in nervemembranes. Certainly, for the body to
The Role of Science
heal damaged nerves (i.e. neuropathy),
function and structure.
The basis of science is manipulating one
omega fatty acids should be in abundant
variable at a time and measuring the re-
supply. When it comes to nerves, the
sult as manifest by another single variable.
proper balance of omega fatty acids can
TENS, SCS, etc. are used throughout Med-
Applying science to the function of an in-
reconstitute the walls of irritated and
icine. The scientific basis for electric
dividual variable, such as nutritionals, is
damaged sympathetic C-fibers. Healthy
nerve blocks has previously been reviewed
antithecal to actual pain presentation.
nerve membranes may very well equal
Real-world patient presentation is very
more normal nerve function.
Intra-cellular changes21 are most likely
complex and involves multiple variables
DL phenylalanine has been shown to
promoted by so-called medium frequen-
working synergistically or antagonistical-
facilitate the production of endorphins in
cy alternating current applied along body
ly to give multiple results of interest.
humans. Since it is an essential amino
parts where cellular dysfunction occurs,
Certainly science helps physicians ob-
acid, it could very well be an ingredient
and nutritionals. We cannot rule out the
jectively analyze things happening in
in the endorphin recipe.28
importance of changes in intracellular
health care world around us. However,
Vitamin B6 is well-known biochemical-
chemistry that are caused by stress and
many physicians, especially those with re-
ly to be a co-enzyme in the energy cycle.
other psychological phenomena.
search training and advanced scientific
Energy is required for metabolism. Heal-
For best results, the right diagnoses are
degrees, recognize that a very small per-
ing is a metabolic process. It has been
necessary so that the specific pathology
centage of clinical medicine is based on
used for years by general practitioners
can be treated and the electrodes correct-
scientific, double-blinded, controlled,
and nutritional experts for various kinds
ly placed. Treatment history also can have
peer-reviewed proof. Certainly, no such
of soft tissue pain.
unanticipated results. For example, multi-
evidence exists for the effectiveness of ap-
The association between vitamin B12
ple previous chemical blocks — resulting
pendectomies. Deductive reasoning and
and abnormal fatty acid synthesis pro-
in chemical-induced scar tissue around
experience allows physicians to accept
Practical PAIN MANAGEMENT, Jan/Feb 2003
and use this surgical technique as the
pathology towards a cure rather than
romusculoskeletal Pain taken from Chapters 7 & 13.
"standard of care."
Myofascial Pain and Fibromyalgia: Trigger Point Man-agement. 2nd Edition. Rachlin, ES. and Rachlin, IS.
Logic and scientific information can be
With the realization that pathology,
(eds.) Mosby. 2001.
applied and the results can be valuable
particular in chronic pain, can involve no-
10. Main CJ and Spanswick CC. Pain Management:
without a rigorous scientific experiment
ciceptive, neuropathic and perceptron
An Interdisciplinary Approach. Churchill Livingstone.
New York. 2000. 438 pp.
being done. In fact, the real world of med-
(central) pathology together and in com-
11. Trowbridge HO and Emling RC. Inflammation: A
icine is not a place where "real" science
plex individually varying patterns, inte-
Review of the Process. 5th Edition. Quintessence
can be done, because the real world is
grated medical treatment is the only way
Books. Carol Stream, Ill. 1997. 236 pp.
complex and the best medicine is prac-
to have reasonable hope of optimizing
12. Woessner J. Blocking out the Pain. Practical Pain
ticed on individuals — not populations.
pain care. These pain conditions can be
Management. Mar/Apr 2002. pp. 19-24.
The population approach, based on the
so complex that we fully expect a new field
13. Gunn CC. Treating Myofascial Pain: IntramuscularStimulation (Ims for Myofascial Pain Syndromes of
mathematics of statistics, has spawned
of medicine to be developed, such as Pain
Neuropathic Origin). Churchill Livingstone. NY. 1996.
"guidelines," "protocols" and "hard-and-
14. Reeves KD. Prolotherapy: Basic Science Clinical
fast" rules. "Protocols" are helpful, but
Each of the opinions stated above can
Studies and Technique. Lennard Pain Procedures inClinical Practice. Hanley and Belfus Inc. Phila. 2000.
should not be controlling.
be supported from the published litera-
15. Linetsky FS, et al. (editors) Position Paper: Re-
ture; however, a careful presentation of
generative Injection Therapy (RIT): Effectiveness and
the arguments on both sides would re-
Appropriate Usage. The Florida Academy of Pain
Care As a Beginning
quire publication of several books. The in-
Medicine (FAPM). 2001. 12 pp.
Integrated or Blended Medicine is a con-
tent here is to stimulate new and more
16. Miyoshi HR. 2001. Systemic Nonopioid Anal-gesics. Bonica's Management of Pain. 3rd Edition.
cept that is gaining credence in recent
correct approaches in fashioning a cus-
Loeser, et al. (editors). Lippincott, Williams & Wilkins.
years. Clinics are including "integrated"
tom solution for individual patients to at-
Philadelphia. pp. 1667-81.
in their names. Understanding that the
tempt cure or, at the very least, improve
17. Max MB and Gilron IH. Antidepressants, Muscle
CAM portion of Integrated Medicine is
their condition. I
Relaxants, and N-Methyl-D-Asparatate Receptor An-tagonists. Bonica's Management of Pain. 3rd Edition.
still in its infancy (in a scientific sense) log-
Loeser, et al. (editors). Lippincott, Williams & Wilkins.
ically means that Integrated Medicine
Dr. James Woessner holds a doctorate in bio-
Philadelphia. 2001. pp. 1710-26.
must also be in its infancy. However, in the
logical sciences in conjunction with a medical
18. Childers MK. Use of Alpha-2 Adrenergic Agonists
opinion of the author, this is the direction
degree. His professional medical training in-
in Pain Management. Academic Information Systems.
2001. 128 pp.
that is most likely to advance pain care,
cludes neurology and physiatry. Dr. Woessner
19. Rowbothan MC and Petersen KL. Anticonvulsants
now and in the future.
collects and analyzes data on a daily basis in
and Local Anesthetic Drugs. In Loeser, et al. (eds.)
his multidisciplinary practice; he frequently
Bonica's Management of Pain. 3rd Edition. Lippincott,
Synthesis, Summary and Conclusions
writes and lectures about pain and other sub-
Williams & Wilkins. Philadelphia. 2001. pp. 1727-35.100
With this conceptual model of pain, we
jects in Physical Medicine. Dr. Woessner may
20. Brookoff D. Chronic Pain: 1. A New Disease?
have described a practical and more direct
be contacted at Advanced Phys Med, 2615
Hospital Practice. The McGraw-Hill Companies. Web-
way of analyzing the function of small pain
22nd St., Lubbock, TX 79410; 806-687-
nerves. Deductively, depending on the
5420. [Editor's note: Dr. Woessner is in the
21. Knedlitscheck G. et al. Cyclic AMP response incells exposed to electric fields of different frequen-
pattern and consistency of dysfunction,
process of relocating to California and new con-
cies and intensities. Radiation Environmental Bio-
neuropathic and central pain can now be
tact information will be made available by con-
physics. 1994. 32:1-7.
analyzed in a more logical fashion.
tacting Practical Pain Management.]
22. Zhou L, Ming L, and Jiang Q. [Protective effect of
Medicine, particularly allopathic med-
extract of folium ginkgo on repeated cerebral is-chemia-reperfusion injury] in Chinese. Zhongguo
icine, has concentrated on curing noci-
References
1. Woessner J. A Conceptual Model of Pain. Practical
Zhong Xi Yi Jie He Za Zhi. May 2000. 20(5):356-8.
ceptive pain, i.e., removing the patholo-
Pain Management. Sept/Oct 2002. 2:5, 8-16, 37.
23. McCabe S. Complementary herbal and alterna-
gy. Meanwhile, Oriental Medicine and
2. Woessner J. A Conceptual Model of Pain: Mea-
tive drugs in clinical practice. Perspect Psychiatr
CAM have — serendipitously — dealt with
surement and Diagnosis. Practical Pain management.
Care. Jul-Sep 2002. 38(3):98-107.
dysfunction of the sympathetic nervous
Nov/Dec 2002. pp. 2 735.
24. Baron R and Wasner G. Complex regional painsyndromes. Curr Pain Headache Rep. Apr 2001.
system of which the C-fibers are a part.
3. Bonica JJ and Loeser JD. Applied Anatomy Rele-vant to Pain. Bonica's Management of Pain. 3rd Edi-
Medicine as a whole should integrate the
tion. Loeser, et al. (eds.). Lippincott, Williams &
25. Juhan D. A Handbook for Bodywork: Job's Body.
best of CAM, Oriental and Western Med-
Wilkins. Philadelphia, PA. 2001. pp. 196-221.
Barrytown, Ltd. New York. 1998. 412pp.
icine to push forward with the curative
4. Hackett GS. Ligament and Tendon Relaxation
26. Anonymous. The Impact of Chronic Pain-An Inter-
(Skeletal Disability) Treated by Prolotherapy (Fibro-Os-
disciplinary Perspective. Purdue Pharma. June 2000.
practice of Pain Medicine.
seous Proliferation). 3rd Edition. Charles C. Thomas.
CAM and Oriental Medicine treatments
Springfield, IL. 1958. 151 pp.
27. Anonymous. Managing Chronic Pain in Ten Easy
that mostly did not make "sense" in the
5. Travell J and Simons D. The Trigger Point Manual.
Steps. Copyright Pain Association Scotland. Edin-
past, are starting to make "sense" now as
Volume I. 1994.
burgh, Scotland. 2 pp. Reprinted with permission.
we learn more. These treatments include
6. Travell J and Simons D. The Trigger Point Manual.
28. Russell AL and McCarty MF. DL-phenylalanine
Volume II. 1994.
markedly potentiates opiate analgesia - an example
"tissue remolding," psychophysiological
7. Hooshmand H. Chronic Pain: Reflex Sympathetic
of nutrient/pharmaceutical up-regulation of the en-
(mind-body), electrical, herbal and nutri-
Dystrophy, Prevention and Management. CRC Press.
dogenous analgesia system. Med Hypotheses. Oct
tional approaches. With these integrative
Boca Raton, FL. 2000. 202 pp. Figure reprinted with
2000. 55(4):283-8.
approaches and scientific deduction, it is
29. Bodger C. Smart Guide to Healing Back Pain.
8. Butler DS. Mobilisation of the Nervous System.
John Wiley & Sons. New York. 1999. 229 pp.
becoming increasingly clear that physi-
Churchill Livingstone. New York. 1991. 265 pp.
30. Peilin S. The Treatment of Pain with Chinese
cians can begin retarding, maintaining,
9. Fischer AA. Segmental Neuromyotherapy: A New
Herbs and Acupuncture. Churchill Livingstone. New
and regressing neuropathic and central
Concept in the Diagnosis and Management of Neu-
York. 2002. 656 pp.
Practical PAIN MANAGEMENT, Jan/Feb 2003
Source: http://electromedicine.org.au/wp-content/uploads/2014/01/Pain-Model-03.pdf
What's New in Veterinary Dermatology Anthea Schick, DVM, DACVD Every spring, the American College of Veterinary Dermatology (ACVD) and the American Academy of Veterinary Dermatology (AAVD) host a North American Veterinary Dermatology Forum (NAVDF). This April the NAVDF was held in Nashville, TN. The NAVDF is open to everyone with an interest in
FRiDAY EvEning, DEcEMbER 4, 2015 Torah Portion – Vayigash Genesis 44:18 – 47:27 Haftarah – Ezekiel 37:15 – 28 Shabbat Goes Disco Services Shabbat Services 2 7:30 p.m. Disco Dinner and Dancing FRiDAY EvEning, DEcEMbER 25, 2015 SATuRDAY, DEcEMbER 5, 2015 From Strength to Strength 4 9:00 a.m. Torah Study Clergy's Corner 5 10:30 a.m. Morning Minyan5:30 p.m. Bar Mitzvah of Ari Romano



