Viagra gibt es mittlerweile nicht nur als Original, sondern auch in Form von Generika. Diese enthalten denselben Wirkstoff Sildenafil. Patienten suchen deshalb nach viagra generika schweiz, um ein günstigeres Präparat zu finden. Unterschiede bestehen oft nur in Verpackung und Preis.
Bmjopen-2011-000195 1.7
Introduction and evaluation of a
‘pre-ART care' service in Swaziland:an operational research study
David Burtle,1 William Welfare,2 Susan Elden,2 Canaan Mamvura,2Joris Vandelanotte,3 Emily Petherick,4 John Walley,1 John Wright4
To cite: Burtle D, Welfare W,
Elden S, et al. Introduction
Objective: To implement and evaluate a formal
and evaluation of a ‘pre-ART
pre-antiretroviral therapy (ART) care service at
care' service in Swaziland: an
a district hospital in Swaziland.
- Impact of pre-ART care on the quality of care in
operational research study.
Design: Operational research.
BMJ Open 2012;2:e000195.
a district hospital in Southern Africa.
Setting: District hospital in Southern Africa.
Participants: 1171 patients with a previous diagnosis
- After introduction of a pre-ART care service,
of HIV. A baseline patient group consisted of the first
< Prepublication history for
a higher proportion of patients were assessed for
200 patients using the service. Two follow-up groups
this paper is available online.
ART, a higher proportion of those eligible started
were defined: group 1 was all patients recruited from
To view these files please
on ART and a higher proportion received key
April to June 2009 and group 2 was 200 patients
visit the journal online (http://
recruited in February 2010.
Intervention: Introduction of pre-ART careda package
Strengths and limitations of this study
of interventions, including counselling; regular review;
- This was a pragmatic evaluation in a routine
DB and WSW contributed
clinical staging; timely initiation of ART; social and
service setting.
equally to this work.
psychological support; and prevention and management
- The intervention was implemented as part of
of opportunistic infections, such as tuberculosis.
routine health service delivery by existing clinical
Received 26 May 2011
Primary and secondary outcome
Accepted 1 February 2012
measures: Proportion of patients assessed for ART
- Routine data collection systems do not link
This final article is available
eligibility, proportion of eligible patients who were
testing and HIV care data, preventing an
for use under the terms of
started on ART and proportion receiving defined
evaluation from testing to initiation.
the Creative Commons
evidence-based interventions (including prophylactic
- The evaluation focuses on those with a known
co-trimoxazole and tuberculosis screening).
status, rather than new testers, those with
Results: Following the implementation of the pre-ART
tuberculosis or those who are pregnant.
service, the proportion of patients receiving defined
- The evaluation relies on intermediate outcomes,
interventions increased; the proportion of patient being
that is, initiation on ART, rather than long-term
assessed for ART eligibility significantly increased
outcomes, such as mortality.
(baseline: 59%, group 1: 64%, group 2: 76%;
- There is a lack of information on those requiring
p¼0.001); the proportion of ART-eligible patients
long-term follow-up but not ART.
starting treatment increased (baseline: 53%, group 1:81%, group: 2, 81%; p<0.001) and the median time
between patients being declared eligible for ART and
Mortality rates of between 8% and 26% have
Nuffield Centre for
initiation of treatment significantly decreased (baseline:
International Health and
61 days, group 1: 39 days, group 2: 14 days; p<0.001).
been reported,1 with advanced immunodefi-
Development, Leeds Institute
Conclusions: This intervention was part of a shift in
ciency as a key risk factor.2 High rates of loss
of Health Sciences,
the model of care from a fragmented acute care model
to follow-up after HIV testing result in late
University of Leeds, Leeds,
to a more comprehensive service. The introduction of
presentation for ART initiation and are
structured pre-ART was associated with significant
associated with poor treatment outcomes.3 4
Good Shepherd Hospital,
improvements in the assessment, management and
In light of the negative outcomes associated
Siteki, Swaziland3
timeliness of initiation of treatment for patients with
ICAP Swaziland, Mbabane,
with late presentation, there has been
a renewed focus on the period after HIV
4Bradford Institute for Health
diagnosis but before commencement of
Research, Bradford Teaching
treatment.5 Numerous studies have investi-
Hospitals NHS Foundation
gated retention of patients following HIV
Trust, Bradford, UK
diagnosis.3 4 6e23 Rates of enrolment of
Correspondence to
In sub-Saharan Africa, HIV-positive adults
eligible patients on ART vary widely (14%e
William Swithun Welfare;
have a high mortality rate during the first
84%), and retention of patients not yet
Burtle D, Welfare W, Elden S, et al. BMJ Open 2012;2:e000195. doi:10.1136/bmjopen-2011-000195
Pre-ART service evaluation
eligible for ART treatment remains very challenging in
estimated at 26%.27 The Swazi National Strategic
many of these settings (45%e70%, though the majority
Framework for HIV and AIDS 2009e2014 recommends
of these studies did not provide data for those with HIV
structured pre-ART care as part of a three pronged
but not on ART). Asymptomatic patients, not yet eligible
treatment strategy along with increasing HIV testing and
for ART, may not appreciate the need for medical care at
the expansion of ART provision.28 The framework
this stage and may be put off by the disruption, expense
recognised that pre-ART care was in ‘its infancy', with
and stigma of repeated clinic visits for, what they
a limited number of sites providing this package at the
perceive as, little treatment.5 Patients with low CD4 cell
counts at presentation may die before presentation and
Good Shepherd Hospital (GSH) is the district referral
so not complete ART enrolment.
There is emerging evidence of the relative success of
a predominantly rural area of approximately 250 000
different approaches to improve retention during this
period. These include rapid clinical staging through the
Prior to the introduction of the pre-ART care service in
use of point of care CD4 tests24 and the implementation
February 2009, HIV care prior to commencing ART at
of more coherent care pathways.5 There remains a need
our institution was episodic. There was no continuum of
for a clearer understanding of how to improve patient
care, and patients were only followed up consistently
retention at this point in resource-poor settings.
once they were started on ART. Patients with unknownstatus were tested in the HIV testing and counselling
centre. If found to be HIV positive, a sample was taken
Pre-ART care spans the period between a person testing
for CD4 testing and they were instructed to return to the
positive for HIV and needing ART. For some people, this
separate ART centre in 3 days to collect the result. If they
is very short, just the time for assessment, while for
returned, they received counselling, TB screening,
others, this could be a period of years. A short period of
co-trimoxazole and further appointments as necessary.
pre-ART may result from delayed presentation for
An internal audit of services in October 2008 revealed
testing or a delay between receiving the initial test result
and receiving (or seeking) HIV care. During the pre-
< Over 1/3 (153/407) of pre-ART hospital patients did
ART period, a number of interventions can improve the
not return to collect CD4 counts and therefore
health of people living with HIV and provide an effective
received no follow-up.
pathway to ART for those who require it.25 26
< Patients started ART late, the median CD4 at first test
was 116 cells/mm3.
The components of a pre-ART care service
< Although co-trimoxazole was prescribed for pre-ART
< Assessment for ART.
patients, there was no system of receiving a regular
– Regular follow-up and review.
supply of this.
– Assessment for ART, including clinical staging, CD4,
< HIV counsellors stated that they performed TB
biochemistry and haematology.
screening, but it was not offered systematically nor
– Initiation for ART when agreed criteria are met.
recorded or nor was there a system to follow-up
Creation of the pre-ART care service linked hospital
Opportunistic Infections (including co-trimoxazole
HIV testing and ART services and aimed to improve
and isoniazid prophylaxis, and tuberculosis (TB)
patient follow-up by formalising previously fragmented
– Counselling including advice to prevent onward
transmission of HIV (including promotion of
condoms) and promote testing of those at risk25 26
The service design drew on the following concepts:
< Comprehensive care: using a patient care pathway.
< Active follow-up: structured follow-up by cell phone
The aim of this study was to implement and evaluate
and adherence officers.
a formal pre-ART care service at a district hospital in
< Task shifting: to nurses and lay HIV counsellors.
Swaziland. The pre-ART service aimed to increase thekey outcomes of:
Comprehensive care
< assessment of patients for ART eligibility;
Staff plotted the patient pathway from HIV testing to
< initiation of those eligible on drug treatment;
ART treatment. Service gaps along this pathway were
< provision of evidence based interventions to improve
identified and quantified. Monthly meetings were held
with staff to review performance and develop the service.
Three records were introduced: (1) inpatient pre-ART
file, (2) patient handheld file and (3) pre-ART registra-
The Kingdom of Swaziland is suffering a ‘hyper-
tion book. The inpatient file was a way of documenting
epidemic' of HIV infection with adult prevalence
a comprehensive and systematic care plan for each
Burtle D, Welfare W, Elden S, et al. BMJ Open 2012;2:e000195. doi:10.1136/bmjopen-2011-000195
Pre-ART service evaluation
patient. The patient handheld file enabled patients totake greater responsibility for their care and to improvethe continuity of care if patients presented at otherfacilities. The pre-ART registration book enabled follow-up when patients did not return for their appointmentsand monitoring of system performance.
Active follow-upPatients who did not return for appointment werecontacted by phone. Reasons for not returning wereidentified. Those who could not be reached by phonewere followed up by the motorcycle adherence officers attheir homes as part of a pre-existing service supportingHIV, TB and epilepsy services.
Task shifting to nurses and HIV counsellorsIn common with many rural HIV health services inSouthern Africa, the service demands outstripped thehuman resource capacity. When the pre-ART servicestarted in February 2009, the staff for the HIV serviceconsisted of two doctors, two nurses, three HIV coun-sellors and one pharmacist to attend to an average of2000 patients each month. Previously assessment forART initiation was doctor-led. The new pre-ART servicewas nurse-led. Nurses provided the triage for patientsentering the pre-ART system and most of the clinicalassessment for ART initiation. At the time of the analysis,only physicians were allowed to initiate ART drugs,
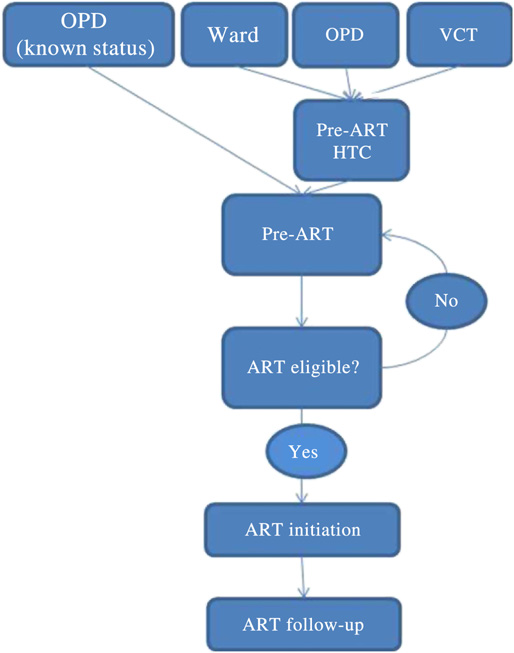
Flow diagram outlining the current (new) HIV
creating a bottleneck. Task shifting, including nurses
pathway at Good Shepherd Hospital. ART, antiretroviral
seeing majority of review patients and undertaking
therapy; ART eligible?, definition based on the standardised
pre-ART, freed up time for doctors to initiate ART.
WHO criteria; OPD, outpatients department; OPD (knownstatus), patients known to be HIV positive presenting to the
HIV counsellors took on additional roles of TB
outpatient department; pre-ART HTC, HIV testing and
screening and phlebotomy from the nurses. Task shifting
counselling as part of pre-ART care; VCT, Hospital Voluntary
to nurses and HIV counsellors reduced the number of
Counselling and Testing Service; ward, general hospital wards.
steps in the patient pathway, improved the efficiency andmade the most effective use of limited resources.
formed the population for this study. This register didnot include data from new testers, those who were
pregnant or were known to be co-infected with TB.
A structured pre-ART care service was established at GSH
These groups were entered in other registers. Data were
in January 2009. The patient flow created is shown in
entered in a Microsoft Excel 2007 spreadsheet. Three
groups were defined:
The interventions were based on the WHO guidance.
Baseline: 200 patients, February to March 2009, the first
When the service was started, there were no national
patients enrolled by the service
pre-ART guidelines, although recently a Swaziland
Group 1: 771 patients, April and June 2009, to assess the
comprehensive package of care has been published.
impact of the initial service implementation.
Interventions provided as part of pre-ART care at this
Group 2: 200 patients, February 2010, to assess the
hospital included: baseline laboratory testing, CD4 cell
impact of the service after 1 year.
count, initial clinical review and staging, regular reviewevery 3 or 6 months, TB symptom screening, manage-
Data were collected from the pre-ART register in June
prophylaxis and referral to the ART service when indi-
2010. All patients had at least 3 month follow-up.
cated. During the study, isoniazid chemoprophylaxis wasnot in routine use in Swaziland.
AnalysisDifferences in baseline values between the three groups
EVALUATION METHOD
were examined using analysis of variance for continuous
variables and c2 tests for differences in proportions.
Patients with a known diagnosis were registered for the
Comparisons between outcomes in groups were
pre-ART service in the ART department and these
examined between the groups using c2 tests and
Burtle D, Welfare W, Elden S, et al. BMJ Open 2012;2:e000195. doi:10.1136/bmjopen-2011-000195
Pre-ART service evaluation
a comparison of performance indicators using c2 tests
management and care significantly improved over the
for differences in proportions and KruskaleWallis test to
study period. The proportions of patients being assessed
look at differences in time between ART initiation in
for ART eligibility and ART-eligible patients starting
eligible patients between groups, using STATA IC 11.2.
treatment significantly increased; the time between
The level of statistical significance was set at 5%.
PLHIV being declared eligible for ART and them
The key outcomes analysed were as follows:
starting ART significantly decreased. The proportion
The proportion of patients with a documented assess-
being assessed for ART remains lower than ideal. A
ment of eligibility for ART initiation (including clinical
significant proportion of patients are testing positive,
stage, CD4 count and baseline biochemical and haema-
being registered for pre-ART, but then not returning for
tological testing) among patients recruited to the
CD4 count results. Eligible patients commencing ART
pre-ART service.
more rapidly is important given the very high mortality
The proportion of patients started on ART among those
risk immediately prior to starting ART.1 2
eligible for ART initiation.
The trend in proportion of patients on co-trimoxazole
The proportion of patients who received specified
is less clear. The supply of co-trimoxazole was dependent
interventions (TB screening, initial CD4 count, clinical
on the national system and out of the control of the
staging, assessment of eligibility for ART and co-trimox-
service. Problems with consistent supplies of co-trimox-
azole prophylaxis), as part of pre-ART care.
azole and non-implementation of isoniazid prophylaxisare commonly recognised issues in resource-limitedsettings.29
RESULTSThe demographics of the three groups reflect largely
Strengths and limitations of the study
similar populations (table 1), although the proportion
This study provides timely evidence about the impact of
with CD4 counts under 200 and under 350 cells/mm3
a clinical intervention for a public health priority. The
increased in each of the three groups, and the median
findings are likely to be generalisable to other low-
CD4 count was found to decrease in each of the groups.
resource settings where the prevalence of HIV/AIDS is
The service's performance in assessing patients for
high. The intervention was implemented as part of
ART eligibility and then initiating those eligible is shown
routine health service delivery by existing clinical staff,
in table 2. The proportions of People living with HIV
promoting sustainability. A randomised controlled trial
(PLHIV) being assessed for ART eligibility and propor-
would provide more robust evidence about effectiveness,
tion of eligible patients being initiated on ART signifi-
but this pragmatic evaluation provides useful evidence
cantly increased in each group (c2 for variance, ps
on how to improve care in a setting where HIV/AIDS is
0.01). The median time between eligibility and initia-
a national emergency. While this study cannot prove
tion significantly decreased (p<0.01).
causation, it demonstrates an association between the
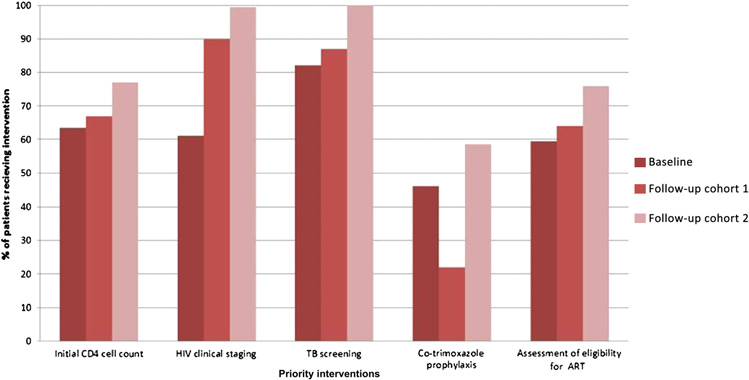
Rates of CD4 cell counting, clinical staging, TB
introduction of the service and improved performance.
screening and ART assessment increased gradually
The implementation of pre-ART care involved a number
between groups (figure 2). The proportion receiving
of changes to HIV services at GSH. It is not possible to
co-trimoxazole prophylaxis fell between baseline and
determine the weight of each changes' contribution.
group 1, reflecting problems with drug supply, but did
The rapid change in performance of the service seen
rise over the 1-year period.
between baseline and group 1 (table 2) suggests thatthe implementation of structured pre-ART care was
associated with improving performance.
Following the introduction of structured pre-ART, the
The reliance on routine data limits the quality of
proportion of patients with HIV receiving appropriate
analysis possible in this study. We were unable to link
Summary of demographic and clinical characteristics of the three groups
p Value comparison
Mean age (SD) (years)
Gender (% female)
Number and proportion of adult patients
with a recorded CD4 count, N (%)Median CD4, range (cells/mm3)
Number and proportion of adult patients
with a CD4 count <350, N (%)Number and proportion of adult patients
with a CD4 count <200, N (%)
Burtle D, Welfare W, Elden S, et al. BMJ Open 2012;2:e000195. doi:10.1136/bmjopen-2011-000195
Pre-ART service evaluation
Comparison table of assessment for ART eligibility and initiation between the three groups
Number assessed for ART/all patients
attended clinic, N (%)Number assessed eligible for ART/
number assessed for ART, N (%)Number of eligible patients initiated
on ART/number assessed as eligiblefor ART, N (%)Median time between eligibility and
ART initiation (range) (days)
ART, antiretroviral therapy.
testing data (some of which is anonymous) to pre-ART
Over the study period, the proportion of patients
information. Ideally, we would have followed cohorts of
assessed as eligible has increased. This reflects differ-
patients from testing to initiation, but this was not
ences in health of the groups, as well as changes in
possible. Data were collected from the register in the
international and national guidelines on CD4 threshold
ART department, which is of patients with a known
for initiation. The reasons for increasing numbers of
diagnosis and not those with a new diagnosis. The
patients with advanced immunodeficiency in groups 1
people in this study are therefore likely to have more
and 2 are unclear. This should not have affected the key
advanced immunodeficiency and may not be typical of
outcomes of this study: the proportion of patients
all patients with HIV/AIDS. The data used excludes
assessed for ART and the proportion of those eligible
those who were pregnant or those on TB treatment as
who were initiated.
those services also run parallel pre-ART services. Strati-fying the patient by source of referral and/or testing
Lessons from implementing pre-ART care
(eg, Voluntary counselling and Testing (VCT) or ward or
Implementing a coherent HIV pathway across multiple
outpatients) would be useful, but that information was
programmes within the hospital was a complicated
not routinely recorded.
process. The overall service includes HIV-positive
The differing group sizes resulted from data that had
patients in hospital TB and Prevention of Mother to
been previously entered as part of a pilot evaluation. The
Child Transmission (PMTCT) programmes in addition
researchers opted to use all the available data, rather
to the pathway described above. Integration of separate
than ignoring any of it. The impact of a larger group 2 is
vertical national programmes (eg, PMTCT, TB, ART) at
unclear. A larger group 2 (ie, spanning a longer time
a district level to provide a coherent service and clear
period) may have increased the difference between
pathway is challenging. The recent introduction of
groups 1 and 2 but lessened the difference between
a national integrated package of care for PLHIV may aid
groups 2 and 3.
Comparison of priority
interventions received by the threegroups. Initial CD4 cell count,p¼0.002; HIV clinical staging,p¼0.001; tuberculosis (TB)screening, p<0.001;co-trimoxazole, p<0.001,assessment of eligibility forantiretroviral therapy (ART),p¼0.001.
Burtle D, Welfare W, Elden S, et al. BMJ Open 2012;2:e000195. doi:10.1136/bmjopen-2011-000195
Pre-ART service evaluation
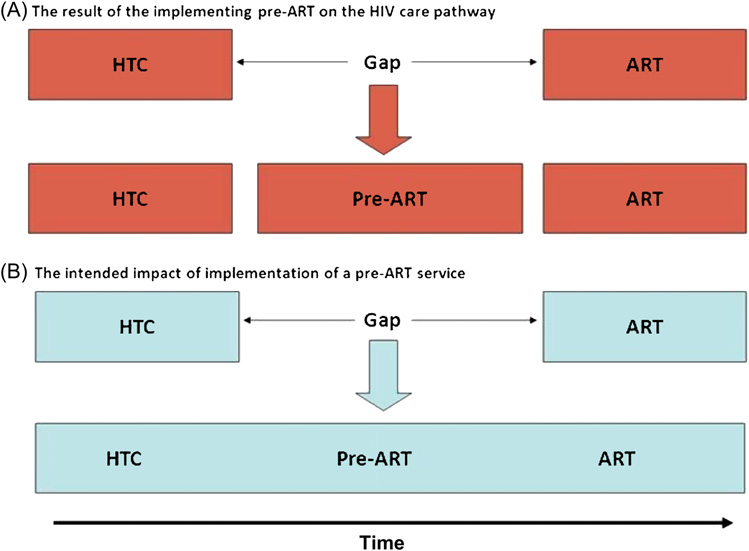
Flow diagram showing
(A) the actual impact of pre-antiretroviral therapy (ART)implementation care pathway and(B) the intended impact. HTC, HIVtesting and counselling.
Problems with monitoring, evaluating and reporting
using paper-based records are well recognised as
The introduction of structured pre-ART was associated
constraining HIV services in other settings.25 30 Separate
‘silos' of information within the HIV programme (such
management and timeliness of initiation of treatment
as separate pre-ART registers) result in independent
for patients with HIV pre-ART care provided the first step
summaries of data about activities that are interrelated
in linking HIV testing and ART services in this rural
and restrict patient monitoring.
African setting. This study suggests that the introduction
The advent and roll-out of ART in low-resource
of a pre-ART service and consequent improved pathway
settings has resulted in a focus on drug treatment to
has been beneficial for patients.
reduce mortality.31 In addition, an emphasis on
Acknowledgements The authors gratefully acknowledge the staff of GSH
increasing knowledge of serostatus has aimed to detect
who both implemented this intervention and supported the evaluation, in
disease earlier and enable people to access ART.32 In
particular Dr Petros (Senior Medical Officer), Mrs Dumsile Simelane, Sister
some areas, this has resulted in a gap in the service
Futhi Ndinisa. The authors also thank the Swaziland National AIDSProgramme, ICAP and the Lubombo Regional Health Management Team for
implementation of HIV care pathwaysdthe link between
their support.
the two.5 17 21 As testing and ART provision increase,
Contributors SE, CM, JV, JWr and JWa devised and implemented the
there will be an increasing group of those with known
intervention. SE and CM undertook data collection and initial evaluation. DB,
infection who need management but not yet ART. Pre-
WSW, JWa, JWr devised the evaluation. DB and WSW undertook the
ART services are key to managing this growing group,
evaluation and initial analysis. EP undertook the statistical analysis. DB, WSW
rather than just being a pathway to ART.
and EP prepared the manuscript. All contributed to revising the manuscript.
Though pre-ART has ‘filled the gap' between, previ-
Funding This document is an output from a project funded by UK Aid from the
ously distinct, HIV testing and ART services, its imple-
UK Department for International Development (DFID) for the benefit of
mentation has produced a system that consists of
developing countries. However, the views expressed and informationcontained in it are not necessarily those of or endorsed by DFID, which can
individual service component services linked together
accept no responsibility for such views or information or for any reliance
(figure 3A), rather than a fully coherent continuum of
placed on them.
care advocated in the literature and standardised
Competing interests None.
protocols (figure 3B).24e26
Decentralisation of HIV services is being implemented
Ethics approval Ethics approval was provided by Swaziland Ministry of HealthScientific and Ethical Committee and University of Leeds.
throughout the Lubombo region.28 This may change therole of the hospital pre-ART service, as chronic HIV
Provenance and peer review Not commissioned; externally peer reviewed.
management is moved to primary care.28 This provides
Data sharing statement Anonymised data on request after review of request
the obvious next step for the service. Operational
by corresponding author ([email protected]).
research is needed to determine the most effective wayto link the hospital and primary care services and the way
Lawn S, Harries A, Anglaret X. Early mortality among adults
in which the current service will change in light of
accessing antiretroviral treatment programmes in Sub-Saharan
Africa. AIDS 2008;22:1897e908.
Burtle D, Welfare W, Elden S, et al. BMJ Open 2012;2:e000195. doi:10.1136/bmjopen-2011-000195
Pre-ART service evaluation
Lawn S, Harries A, Wood R. Strategies to reduce early morbidity and
positive for HIV in South Africa. Bull World Health Organ
mortality in adults receiving antiretroviral therapy in resource limited
settings. Curr Opin HIV AIDS 2010;5:18e26.
Lawn SD, Myer L, Harling, et al. Determinants of mortality and
Larson B, Brennan A, McNamara L, et al. Early loss to follow up after
nondeath losses from an antiretroviral treatment service in South
enrolment in pre-ART care at a large public clinic in Johannesburg,
Africa: implications for program evaluation. Clin Infect Dis
South Africa. Trop Med Int Health 2010;15(Suppl 1):43e7.
Amuron B, Namara G, Birungi J, et al. Mortality and loss to follow-up
Lessells R, Mutevedzi P, Cooke G, et al. Retention in HIV care for
during the pre-treatment period in an antiretroviral therapy
individuals not yet eligible for antiretroviral therapy: rural KwaZulu-
programme under normal health service conditions in Uganda. BMC
Natal, South Africa. J Acquired Immune Defic Syndr 2011;56:
Public Health 2009;9:290e3.
Rosen S, Fox M. Retention in HIV care between testing and treatment in
Losina E, Bassett IV, Giddy J, et al. The "ART" of linkage: pre-
sub-Saharan Africa: a systematic review. PLoS Med 2011;8:e1001056.
treatment loss to care after HIV diagnosis at two PEPFAR sites in
Assefa Y, Van D, Mariam DH, et al. Toward universal access to HIV
Durban, South Africa. PLoS One 2010;5:e9538.
counseling and testing and antiretroviral treatment in Ethiopia: looking
Nsigaye R, Wringe A, Roura, et al. From HIV diagnosis to
beyond HIV testing and ART initiation. AIDS Patient Care STDS
treatment: evaluation of a referral system to promote and monitor
access to antiretroviral therapy in rural Tanzania. J Int AIDS Socirty
Mulissa Z, Jerene D, Lindtjørn B. Patients present earlier and survival
has improved, but pre-ART attrition is high in a six-year HIV cohort
Wanyenze RK, Hahn J, Liechty C, et al. Linkage to HIV care and
data from Ethiopia. PLoS One 2010;5:e13268.
survival following inpatient HIV counseling and testing. AIDS Behav
Karcher H, Omondi A, Odera J, et al. Risk factors for treatment denial
and loss to follow-up in an antiretroviral treatment cohort in Kenya.
Jani I, Sitoe N, Alfai E, et al. Effect of point-of-care CD4 cell count
Trop Med Int Health 2007;12:687e94.
tests on retention of patients and rates of antiretroviral therapy
Tayler-Smith K, Zachariah R, Massaquoi M, et al. Unacceptable
initiation in primary health clinics: an observational cohort study.
attrition among WHO stages 1 and 2 patients in a hospital-based
setting in rural Malawi: can we retain such patients within the general
World Health Organisation HIV/AIDS Department. Priority
health system? Transcripts R Soc Trop Med Hyg 2010;104:313e19.
Intervention for HIV/Aids Prevention, Treatment and Care
Zachariah R, Harries AD, Manzi M, et al. Acceptance of anti-retroviral
in the Health Sector. Geneva: World Health Organisation, 2009.
therapy among patients infected with HIV and tuberculosis in rural
World Health Organisation HIV/AIDS Department. Essential
Malawi is low and associated with cost of transport. PLoS One
Prevention And Care Interventions For Adults And Adolescents Living
With HIV In Resource-Limited Settings. http://www.who.int/hiv/pub/
Micek M, Gimbel-Sherr K, Baptista AJ, et al. Loss to follow-up of adults
plhiv/interventions/en/index.html (accessed 4 May 2011).
in public HIV care systems in central Mozambique: identifying obstacles
Mathabela N, Odido H. Swaziland: Country Progress Report 2010.
to treatment. J Acquired Immune Deficiency Syndr 2009;52:397e405.
April M, Walensky R, Chang Y, et al. Testing rates and outcomes in
country_progress_report_en.pdf (accessed 4 May 2011).
a South African community, 2001e2006: implications for expanded
National Emergency Response Council on HIV and AIDS
screening policies. J Acquir Immune Deficiency Syndr 2009;51:2001e6.
(NERCHA). The National Multisectoral Framework for HIV and AIDS
Bassett IV, Wang B, Chetty S, et al. Loss to care and death before
2009-2014. Mbabane, Swaziland: Government of Swaziland,
antiretroviral therapy in Durban, South Africa. J Acquired Immune
Deficiency Syndr 2009;51:135e9.
Date A, Vitoria M, Granich R, et al. Implementation of co-trimoxazole
Bassett IV, Regan S, Chetty S, et al. Who starts antiretroviral therapy
prophylaxis and isoniazid preventive therapy for people living with
in Durban, South Africa?.not everyone who should. AIDS 2010;24
HIV. Bull World Health Organ 2010;88:253e9.
(Suppl 1):37e44.
Nash D, Batya E, Miriam R, et al. Strategies for more effective
Ingle SM, May M, Uebel K, et al. Outcomes in patients waiting for
monitoring and evaluation systems in HIV programmatic scale-up in
antiretroviral treatment in the Free State Province, South Africa:
resource-limited settings: implications for health systems
prospective linkage study. AIDS 2010;24:2717e25.
strengthening. J Acquired Immune Defic Syndr 2009;52(Suppl 1):
Kaplan R, Orrell C, Zwane E, et al. Loss to follow-up and mortality
among pregnant women referred to a community clinic for
World Health Organisation HIV/AIDS Department. Towards
antiretroviral treatment. AIDS 2010;22:1679e81.
Universal Access. Scaling up Priority HIV/AIDS Interventions
Kranzer K, Zeinecker J, Ginsberg P, et al. Linkage to HIV care and
in the Health sector. Progress Report. Geneva: World Health
antiretroviral therapy in Cape Town, South Africa. PLoS ONE 2010;5:
Organisation, 2009.
World Health Organisation HIV/AIDS Department. Provider-Initiated
Larson BA, Brennan A, McNamara L, et al. Lost opportunities to
Testing and Counselling in Health Facilities. http://www.who.int/pict.
complete CD4+ lymphocyte testing among patients who tested
htm (accessed 4 May 2011).
Burtle D, Welfare W, Elden S, et al. BMJ Open 2012;2:e000195. doi:10.1136/bmjopen-2011-000195
Introduction and evaluation of a 'pre-ART
care' service in Swaziland: an operational
research study
David Burtle, William Welfare, Susan Elden, et al.
BMJ Open 2012 2: doi: 10.1136/bmjopen-2011-000195
Updated information and services can be found at:
These include:
This article cites 26 articles, 1 of which can be accessed free at:
Open Access
This is an open-access article distributed under the terms of theCreative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the originalwork is properly cited, the use is non commercial and is otherwise in compliance with the license. See:http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Receive free email alerts when new articles cite this article. Sign up in
the box at the top right corner of the online article.
Articles on similar topics can be found in the following collections
To request permissions go to:
To order reprints go to:
To subscribe to BMJ go to:
To request permissions go to:
To order reprints go to:
To subscribe to BMJ go to:
Source: http://comdis-hsd.leeds.ac.uk/wp-content/uploads/2013/06/Introduction-and-evaluation-of-a-pre-ART-care-service-in-Swaziland-an-operational-research-study.pdf
Uncaria tomentosa Family: Rubiaceae Common Names: cat's claw, unha de gatoParts Used: Vine bark, root Description Cat's claw (U. tomentosa) is a large, woody vine that derives its name from hook-like thorns that grow along the vine and resemble the claws of a cat. Two closely related species of Uncaria are used almost interchangeably in the rainforests: U. tomentosa and U. guianensis. Both species
BURN WOUND CARE WITH Skin acts as a barrier against infection. CLEANING AND DRESSING YOUR Once you lose your skin, it increases your BURN WOUNDS chance for infection to occur. Taking careof your burn is very important. The • Take pain medication about 30 minutes before following are ways to prevent infection and



